Several pediatric medical conditions have symptoms arising from an allergic response including allergic rhinitis, asthma, food allergy, sting insect allergy, and contact dermatitis (Cox et al., 2008). Allergy skin testing is regularly used as part of the diagnosis process of these conditions (Cox et al., 2008). Immediate Hypersensitivity Skin Test (IHST), a type of allergy skin test, is used to determine specific allergies a person might have based on the way the skin reacts to the test. Children receiving IHST are often advised to not touch or scratch the test site during a 15-minute period, as the test is compromised if the patient touches the test site. After the wait time, the inocutlation site is evaluated, and reaction sensitivity is measured and assessed. A positive sensitivity typically results in a raised, pink area originating at the inoculation site and an itch response that is directly linked to mast cells releasing histamine.
Current Standard of Care for IHST
Children often find the allergy skin tests less painful than immunization and venipuncture. However, the itch sensation caused by a positive reaction can result in distress (Coop & Forester, 2016; Requena et al., 2014; Tahan et al., 2013). Distress is defined as an individual’s evaluation of a taxing situation which is appraised to threaten their well-being and supersede their resources (Lazarus & Folkman, 1984). Common manifestation of distress during an IHST include fear, crying, scratching, or touching the site of the IHST. Patients’ reaction to the testing poses a challenge to the medical team who must prevent the patient from scratching or touching the inoculation site.
During medical procedures such as the IHST, psychological preparation and procedural support are part of the Certified Child Life Specialists’ (CCLS) standard of care to reduce distress, increase coping, and improve compliance (Boles et al., 2020). Psychological preparation utilizes developmentally appropriate explanations to describe the sequence of events, sensory experience, and reason for medical procedures (Child Life Council, Inc., 2011). Interactive distraction is a form of procedural support which requires participants to actively engage in the cognitive process or focus on positive stimuli versus passive observation (Aydin et al., 2016; Kuttner, 2010; Uman et al., 2013).
A systematic review of non-pharmacological pain management techniques supports the use of interactive distraction during procedures to reduce a patient’s distress as well as their perception of pain (Uman et al., 2013). Age-appropriate interactive distraction techniques are routinely used by CCLSs which include, but are not limited to, Look and Find books, light spinners, bubbles, games, and tablets. While many studies have been completed to determine the outcome of these techniques on medical procedures such as venipuncture and intravenous cannulation, few have studied the IHST. Two studies found that psychosocial interventions could be used to decrease pain and anxiety through either musical intervention or medical clowning (Goldberg et al., 2014; Requena et al., 2014). A third observational study found pediatric patients had significantly less distress and more compliance during the IHST if their parents had truthfully informed them about IHST before their medical visit (Tahan et al., 2013). However, none of these studies directly examines the patient’s perception of itch or compares interactive distraction techniques.
Virtual Reality as Interactive Distraction
Interactive distraction (e.g., VR and Look and Find books) is more immersive than passive distraction (e.g., watching a movie or listening to music) because it requires the participant to manipulate the environment, therefore using more attentional resources than a passive task (Jeffs et al., 2014; Pancekauskaitė & Jankauskaitė, 2018; Wickens, 2002). VR is a form of interactive distraction that allows users to experience a world separate from their personal reality. Immersion in a separate reality is achieved by enabling the perception of being physically present in a non-physical world (Lowood, 2020). According to the Multiple Resource Theory, engaging in a task involving one modality (visual) will diminish the individual’s attention resources in another sensory modality (tactile) (Wickens, 2002). Increased levels of immersion in a VR environment captures more of the participants’ attention than simpler forms of distraction (e.g., movies). When a pediatric patient engages in a VR activity, they are utilizing multiple attentional resources (e.g., visual, audio, and cognitive), thus taking away their attention from the negative stimuli. With more attention focused on interactive distraction, less attention would be available for the child to appraise nociceptive inputs, such as pain or itch (Chan et al., 2007). This immersion and interactivity can be accomplished visually with a head-mounted display unit that can present stereoscopic imagery in an environment that isolates the user from the external world by directing the attention to the virtual one.
Many studies have measured the effects of utilizing VR as a form of interactive distraction during medical procedures to decrease the perception of pain and distress with pediatric patients. Studies have shown that VR can have a positive impact on the reduction of perceived pain, pain intensity, unpleasantness, and stress with pediatric patients (Eijlers et al., 2019; Hoffman et al., 2014; Hua et al., 2015; Iannicelli et al., 2019; Law et al., 2011). For example, Hua et al. (2015) found that utilizing VR as a form of interactive distraction decreased pain, decreased distress, and reduced length of time to complete dressing changes in pediatric patients. Few studies have compared VR as a form of interactive distraction to other forms of interactive distraction. A systematic review found it difficult to differentiate the benefits between VR and other types of distraction (Dumoulin et al., 2019; Eijlers et al., 2019; Sil et al., 2012). Additionally, a close examination of the literature revealed that there have been no studies examining the effect of VR distraction on reducing the perception of acute itch nor using VR during IHST.
The purpose of the study was to compare the effectiveness of low-cost VR with the standard of care (e.g., Look and Find and I Spy books) as forms of interactive distraction on increasing patient cooperation and compliance with procedural directives (narrating the sensory stimuli and sequence of events) and reducing patient’s perception of negative procedural outcomes (i.e., itchiness and distress). According to the Multiple Resource Theory, it was hypothesized that VR would increase pediatric patient’s compliance and coping, while decreasing perceived itch and distress during IHST. In addition, a secondary analysis examined impact of age and gender on patient outcomes.
Research Questions
-
Does low-cost VR interactive distraction significantly increase patient’s compliance with IHST and cooperation with procedural directives as compared to the standard of care interactive distraction?
-
Does low-cost VR interactive distraction significantly decrease patient’s perceived itch as compared to the standard of care interactive distraction?
-
Does low-cost VR interactive distraction significantly decrease patient’s distress as compared to the standard of care interactive distraction?
Method
The study was a randomized controlled trial to assess low-cost VR with the standard of care (e.g., Look and Find and I Spy books) as forms of interactive distraction on patient cooperation and patient’s perception of negative procedural outcomes (i.e., itchiness and distress) for pediatric patients receiving IHST.
Sample
Patients between five and 12 years of age seen in the pediatric allergy and immunology clinic at a large quaternary pediatric facility who received a form of IHST were eligible for inclusion in the study. The following types of allergy skin tests were included: adult IHST, child IHST, generic skin test, or allergy and immunology food panel to be placed on the patient’s back. Patients who needed the skin test to be placed on forearms or who needed patch testing were excluded from this study. Patients with epilepsy, visual impairments that would inhibit the use of VR goggles or documented developmental delays that inhibit cognitive or motor capabilities were excluded. All subjects were English-speaking. Caregivers were either English-speaking or Spanish-speaking when an interpreter was available for consent. A patient who spoke a language other than English or a caregiver who spoke a language other than English or Spanish were excluded.
A priori power analysis was done for a comparison of groups itch scores using the Wilcoxon rank-sum test. Under the null hypothesis, the probability is 50% that a randomly selected patient in the experimental group will have an itch score that is lower than a randomly selected patient in the standard of care group. The anticipated 150 subjects per group would have provided 80% power to detect (two-tailed α=0.05) a true increase or decrease of 10% in terms of the probability that a randomly selected patient in the experimental group would have an itch score that is lower than a randomly selected patient in the standard of care group.
Measures
Psychosocial Risk Assessment in Pediatrics (PRAP)
The Psychosocial Risk Assessment in Pediatrics (PRAP) determines the risk of pediatric patient distress during health care encounters (Staab et al., 2014). This scale consists of eight items scored between zero (0) to three (3) with a total score from zero (0) to twenty-four (24). These eight-items include communication, special needs, anxiety and coping during healthcare encounter, temperament, parent/caregiver stress, past healthcare encounter, invasiveness of procedure/encounter, and development impact. It has significant convergent validity with Children’s Emotional Manifestation Scale (CEMS) score (r = .82), parent ratings of patient distress (r = .62), parent ratings of patient cooperation (r = .54), staff ratings of patient distress (r = .69), and staff ratings of cooperation (r= .69). The PRAP has interrater reliability of .985 with 95% confidence interval from 0.980 to 0.980 (Staab et al., 2014).
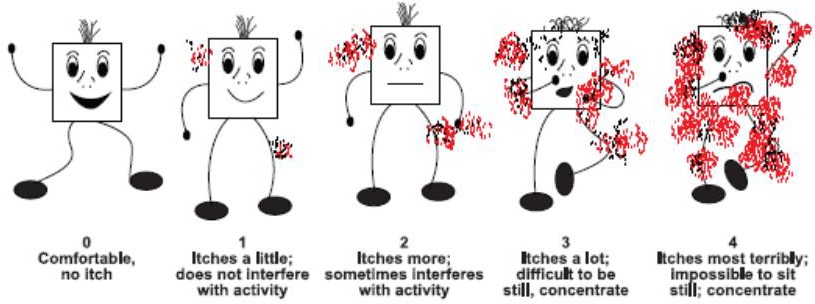
Itch Man Scale
The Itch Man Scale (Blakeney & Marvin, 2000) uses a series of five stick drawings to measure the intensity of itch (Figure 1).
.jpeg)
The measure was developed for an outpatient pediatric burn center and is scored on a 5-point Likert scale with zero (0) representing no itching and four (4) representing intense itching (Blakeney & Marvin, 2000; Morris et al., 2012). This scale has a strong interrater reliability when the scale is administered by two observers to the same patient (r=.91, p<.01). It also correlates significantly with the Visual Analogue Scale (VAS) for itch which is the most frequently used itch assessment (r=.798, p < .0001).
Children’s Emotional Manifestation Scale (CEMS)
The Children’s Emotional Manifestation Scale (CEMS) is an objective, behavioral observation scale used to measure pediatric patient emotional response to stressful healthcare procedures. It consists of five items scored from one (1) to five (5), with the total scores ranging from five (5) to twenty-five (25). The five items include facial expression, vocalization, activity, interaction, and level of cooperation. It has an inter-rater reliability coefficient of 0.96 and the internal consistency of the scale is 0.92 (Li & Lopez, 2005). A positive correlation was reported between CEMS and state anxiety scale (r = 0.76, p < 0.01) with higher levels of state anxiety associated with negative emotional behavior. Inter-rater reliability coefficient of CEMS was reported as 0.96 (Li & Lopez, 2005).
Procedural and Compliance Data
Data regarding procedural directives during the IHST and patient compliance were recorded. The number of times a procedural directive was stated, such as “keep your hands in front of you” or “remember you cannot touch your back,” was recorded. The CCLS also recorded how many times the patient attempted to cross the coronal plane with one or both arms. In addition, the length of time the patient participated in the intervention was recorded. If the patient stopped participating in the intervention, the CCLS recorded the stop time and failure behaviors of the patient. Failure behaviors included no longer responding to procedural directives, no longer responding to re-directive statements from the CCLS, and no longer engaging in either form of distraction.
Data Collection
Prior to initiation of the study, Institutional Review Board approval was received in November 2017. The research team consisted of eight CCLSs who were trained in the research protocol and measures. To ensure consistency of research protocols and data collection methods, the CCLSs practiced obtaining measurements and observed one another prior to the data collection. In the initial design of the study, two CCLSs from the research team were present during the intervention. One CCLS would provide the study intervention and the second CCLS would collect data. Using a tablet, data were collected in REDCap, an electronic research data collection tool. After reviewing a year of data collection experience, CCLSs found they could collect data while performing the intervention. In the fall of 2018, an IRB amendment was approved to have one CCLS provide both the intervention and collect data due to staffing constraints and clinic workflow.
Enrollment
Since the IHST is usually not scheduled in advance, the research team relied on clinic staff to identify potential participants. During the clinic visit, a medical provider determined if a patient needed an IHST and placed the order. After the IHST was ordered, if a patient met the eligibility requirements, clinic staff contacted a CCLS on the research team. A CCLS approached the caregiver and potential subject to explain and discuss participation in the study. Once the caregiver and patient were informed, the CCLS obtained written consent and assent. The CCLS then recorded the sex of the caregiver and rated their stress level using the PRAP.
Each subject was given a unique coded ID which was entered in the patient log with the patient’s name and caregiver’s name in a password-protected file. Using a tablet, data were collected in REDCap. The unique coded ID was used in REDCap to designate the identity of the subject.
Participants were randomly allocated to receive either VR or standard of care as a form of interactive distraction during the test. The PLAN procedure in SAS version 9.4 (SAS Institute., Cary, NC) was used to randomize subjects with block randomization used with a block size of four to ensure that a similar number of subjects was assigned to each group. The study statistician generated the randomization sequence before study enrollment began. Sequentially numbered sealed envelopes contained the group to which the patient was randomized. Only after the patient was consented and enrolled into the study was the envelope opened to reveal the group to which the patient was randomized.
Experimental Group
After enrollment, the CCLS conducted observation and used a caregiver interview to assess the patient using the PRAP (Staab et al., 2014) and made the first CEMS assessment (Li & Lopez, 2005). Next, the CCLS provided psychosocial preparation for the IHST by explaining the sequence of events and sensory experiences based upon the patient’s developmental level and utilized medical equipment to increase understanding. The CCLS explained once the skin test was placed, the patient could not touch their back during a 15-minute wait time to prevent the allergens from being wiped off.
The CCLS introduced VR as an interactive distraction technique to encourage positive coping during the IHST. The CCLS provided Mattel View-Master Virtual Reality goggles. A phone running the Google Expeditions application in “explorer mode” was placed inside the View-Master to enable the immersive, 360-degree imagery the child views. The CCLS explained the VR Google Expedition to the patient and allowed the patient to choose between the expeditions available (e.g., outer space, under the sea, and national parks). The CCLS used an Android v6.x phone and iPod running Google Expeditions in “guide mode” to lead the child on their selected “expedition,” which is a guided tour through VR imagery with descriptions, talking points, and questions.
Immediately before the start of the IHST, the CCLS collected baseline data using the Itch Man Scale (Blakeney & Marvin, 2000). As the nurse applied the IHST, the CCLS began to engage the patient in interactive distraction using VR. The patient did not engage in VR prior to test starting. The CCLS directed the patient’s attention to the VR expedition by asking open-ended questions. In addition, the CCLS narrated the sensory stimuli and sequence of events.
During the IHST, the CCLS tracked the number of times a procedural directive was stated. The CCLS continued to engage the patient in both forms of distraction to re-direct the patient’s attention away from the itchiness of the allergens. The CCLS recorded how many times the patient attempted to cross the coronal plane with one or both arms. The length of time the patient participated in the intervention was recorded. If the patient stopped participating in the intervention, the CCLS recorded the stop time and failure behaviors of the patient. If the patient touched their back, the IHST ended and the CCLS recorded the treatment failure time. When this occurred, the nurse removed the allergens and the CCLS ended the intervention. The patient did not continue forward with the following steps when treatment or distraction failure occurred.
After the 15-minute wait time, the CCLS continued to engage the patient in VR distraction while the nurse measured each allergen. The inoculation site(s) and reaction sensitivity were measured and assessed. The interactive distraction ended after the nurse wiped off the allergens. At the time of IHST completion, patients rated their current perceived itch and their perceived itch during the 15-minute wait time using the Itch Man Scale. The CCLS used the CEMS to rate the patient’s distress during and after the IHST and recorded the number of allergens placed, number of allergens determined to be positive, and whether the patient needed medication to relieve itch after the test.
Standard of Care Group
All study procedures for the standard of care group were replicated from the experimental group, except for the distraction method. For the standard of care distraction, the patient chose between developmentally appropriate Look and Find and/or I Spy books. The standard of care group was offered one type of distraction tool to minimize variability.
Data Analyses
Quantitative variables (i.e., itch score, number of times the patient crossed the coronal plain, number of verbal reinforcements by CCLS, CEMS total, PRAP total, and patient’s age) were compared between groups using the Wilcoxon rank-sum test and categorical variables (i.e., gender, previous allergen test, and use of corrective lenses) were compared using Fisher’s exact test. SAS version 9.4 (SAS Institute Inc., Cary, North Carolina) was used for data analysis. Nonparametric methods were used to avoid the assumption of normality made by the t-test. The primary outcomes were not normally distributed.
Results
A total of 220 patients were enrolled in this study. Of the patients enrolled, 203 patients were eligible for inclusion in the study. Five were excluded after randomization (two for withdrawing and three for not being eligible or not being able to fulfill the study requirements). After initiation, another 12 patients could not complete the study (10/109=9.2% in the experimental group and 2/106=1.9% in the control group, (p = .034), leaving 104 patients in the control group and 99 patients in the experimental group. Those that could not complete the study were due to VR technical failure and/ or showing strong preference to engage in a different distraction method (i.e., personal cell phone or tablet). Most patients were male in both groups and the two groups were similar in age and the proportion of previous allergen tests (Table 1).
None of the outcomes differed significantly for patients in the control versus experimental group (Table 2).
Younger (five to seven years of age) patients crossed the coronal plane more often (p = .003), were given significantly more verbal reinforcements (p = .010), had higher PRAP total scores (p<0.0001), and higher pre-procedure itch scores (p = .018) compared to older (eight to 12 years of age) patients (Table 3).
In stratified analyses comparing sex separately within the two groups, within the experimental group males crossed the coronal plane more often (p = .007), were given significantly more verbal reinforcements (p = .01), and had higher pre-procedure itch scores (p = .005) compared to female patients (Table 4).
Within the control group, males were given significantly more verbal reinforcements by CCLS (p = .028) and had significantly higher (p = .001) during procedure CEMS total scores (Table 5).
In a subgroup analysis of males only, during procedure CEMS total scores were significantly higher (p = .027) for the control group (Table 6).
Discussion
The results of this study showed that the use of low-cost VR as a form of interactive distraction did not significantly increase patients’ cooperation with procedural directives (narrating the sensory stimuli and sequence of events) and did not significantly decrease patients’ perception of negative procedural outcomes (i.e., itchiness and distress) compared to the standard of care (e.g., Look and Find and/or I Spy books). Patients in the VR group were significantly more likely to not complete the test. Patients who did not complete an IHST were then rescheduled for a second attempt thus leading to unnecessary additional exposure to negative stimuli. This could result in higher distress and lack of compliance for pediatric patients.
In further evaluation of the data, the younger ages (five to seven years old) for both the VR and standard of care had less compliance (both reach and verbal redirection), higher PRAP score, and higher pre-procedural itch scores, which were anticipated outcomes based on the children’s development. Despite limited research on the impact of developmental age on coping, younger children often experience magical thinking (in which boundaries are blurred between fantasy and reality) along with the inability to conceptualize time, which can explain why this age group has limited capacity for productive coping (Koller, 2008; Kuttner, 2010).
When comparing sex, boys were significantly less compliant than girls in the VR group in both reach and verbal redirections. In addition, boys required significantly more verbal reinforcements than girls in the standard of care group. Boys also had significantly higher anxiety in the standard of care group compared to girls. Overall, girls were more compliant (did not require as many verbal redirections and attempted to reach for test site less often) compared to boys in both the VR group and standard of care. However, boys in the VR group had lower coping scores compared to the standard of care, although this difference was not statistically significant. It is often assumed that boys gravitate more towards technology; however, there is no specific research to support this (Koller, 2008). CCLS’s should individually assess the patient to determine specific interests to aid in interactive distraction when utilizing VR or other forms of technology. More research is needed to determine the impact of sex on patient’s coping and compliance with medical procedures.
Despite VR being a novel technology, the study shows it has similar outcomes compared to other forms of interactive distraction in terms of patient compliance, coping, and perceived itch. Similarly, previous studies showed no significant difference in reported pain and fear when comparing VR to other forms of interactive distraction during IV, blood draws, and cold pressure trials (Dumoulin et al., 2019; Eijlers et al., 2019; Sil et al., 2012). These results do not support the Multiple Resource Theory, given that VR increases the level of immersion, capturing more of the participants’ attention than simpler forms of distraction. As previously stated, CCLSs utilize other distraction techniques that are less costly and require less maintenance (e.g., charging, Wi-Fi connectivity, IOS updates, and overall durability of product). Without statistically significant results demonstrating that VR increases compliance and decreased distress, we do not recommend low-cost VR as a form of interactive distraction for CCLSs in the hospital setting. More studies need to be done comparing low-cost versus high-end VR (e.g., strap on goggles with headphones, technology support team, and applications that were developed for hospitalized children).
While both groups received preparation for the IHST, a previous study noted the positive effect of preparation on coping with the IHST (Tahan et al., 2013). Future studies should explore the relationship and effectiveness of psychological preparation and interactive distraction on itch, compliance, and distress to better tailor interventions. The inclusion of a control group utilizing passive distraction or a VR intervention without CCLS interaction may better elucidate the difference between interventions and their effects. This information would allow CCLSs to provide better assessments and allocate limited resources.
Limitations
This study has several limitations. Neither the patients nor researchers were blinded to the research condition. CCLSs knowing the purpose of the study may have introduced biases and influenced results. During the consent, patients were informed of VR being a possibility during IHST and occasionally verbalized disappointment or excitement after learning their group assignment. Each patient’s personal bias over novel technology may have affected their level of engagement during the procedure. This was particularly challenging for this team of CCLSs as their role in the hospital setting is to provide choices to enhance the patient’s sense of control and cater to the patient’s interests. When a patient is not enrolled in the study, the patient would have choices between multiple distraction modalities and the freedom to move between them during the procedure. Future studies may consider enrolling patients based on their interest in VR technology instead of randomization, which could alter the impact of attention towards the provided distraction method.
As the study took four years to complete, the low-cost VR technology (both the iPod and the application) became outdated which required updates to the application, hindering enrollment of participants into the study for a period. Also, due to the location of the clinic being in a large facility, the Wi-Fi connectivity was poor and often unreliable. This led to needing to obtain a Wi-Fi hotspot to improve connectivity. As a result of these limitations, the team of CCLSs is hesitant to recommend low-cost, cellphone-based VR. Consistent updates and additional requirements of applications, along with challenging Wi-Fi connectivity, required the CCLSs to focus large amounts of time on technical support that would have otherwise been focused on patient care. This study did, however, only used one form of low-cost VR. Additional studies should be conducted to see if it would yield similar results with other types of low-cost VR.
Another limitation was the Allergy and Immunology Clinic workflow. It was a busy clinic, and the study enrollment often was perceived as a delay of the clinic schedule. On busy days, nursing staff did not feel there was time to consult a CCLS and wait for consent. Therefore, they completed the procedure without study enrollment. This inevitably led to a smaller sample size than originally desired. Also, the CCLS team experienced prolonged staffing challenges among the team of investigators, which significantly limited the availability of CCLSs to obtain consents. For example, the CCLS remained at the bedside during the 15-minute wait time, which is not the normal clinic workflow. If patients were coping appropriately, the CCLS historically would leave the exam room after the allergens were placed to allow them to meet the high demand of IHSTs being placed.
Due to the clinic workflow and staffing challenges, the research protocol was altered mid-study from having two CCLSs present (one CCLS providing child life services and one CCLS collecting research data) to one CCLS who completed both elements of the intervention and data collection. The CCLS had to consistently redirect their focus between assessment, intervention, and data collection. This could have been a limiting factor because the CCLS could not fully devote their attention to distracting patients.
An additional limitation was the Itch Man Scale was originally intended to be used with patients who have burn injuries. Despite this, after extensive searching, this was the only scale that was found to measure perceived acute itch of any form. For this study, the measurement was used for patients experiencing itch due to IHST.
Conclusion
The findings of this study demonstrate that VR had similar outcomes compared to other forms of interactive distraction in terms of patients’ compliance, coping, and perceived itch. More studies are necessary to determine children’s response to VR at different developmental ages to improve the outcomes of interventions. Future research should take into consideration the participant’s developmental age as there are no specific recommendations for age and time usage with VR technology. The American Academy of Pediatrics (2016) has standards regarding appropriate age and exposure levels of screen time for children and adolescents; however, there is no specific policy that outlines the use of VR as a form of entertainment for this age range. In addition to cognitive development, physical development needs to be taken into consideration. The movement required on behalf of the participant to use VR in correlation with the procedure and the surrounding environment needs to be considered when using VR as a form of distraction in the pediatric hospital setting.
Few studies have compared VR to other forms of interactive distraction, more specifically interactive distraction provided by a CCLS. One study, however, did compare VR (without the support of a CCLS) to distraction provided by a CCLS during needle related procedures (Dumoulin et al., 2019). The pediatric patients demonstrated a significant reduction in fear but not in pain in the VR group compared to the distraction provided by a CCLS (Dumoulin et al., 2019). Future studies should be performed in which VR is used as a form of interactive distraction with and without the support (e.g., preparation and procedural support) of a CCLS.
With the advancement of technology, the field of child life has limited research supporting new forms of distraction. This team of CCLSs struggled to find independent research (not sponsored by a company) that compared new technology to traditional child life interventions. Further research is vital for the advancement of the child life profession within the medical community.
Acknowledgements
First, we would like to thank Andrew Peterman for fulfilling our technical support needs. Without your knowledge and expertise, this study would not have been a success. Additionally, we would also like to thank the following Certified Child Life Specialists who aided in data collection: Lesley Chong, Kara Knodel, Kimberly Leatherwood, Casey Page-Jones, and Holly Stanley.