Certified child life specialists (CCLS) reduce the adverse impacts of childhood hospitalization through evidence-based practices, such as play, diagnosis education, and procedural preparation and support (Diener et al., 2018; Grissom et al., 2016; Hyland et al., 2015; Romito et al., 2021). The positive impact of child life services may partially be attributed to the relationships that CCLS build with their patients (Boles et al., 2020; Cole et al., 2001; Turner & Fralic, 2009). Clinical relationships in child life are both supportive and therapeutic, combining warmth and emotional support with a focus on addressing a specific patient need or concern (McCue, 2018). Such aspects of the CCLS-patient relationships are similar to aspects of teacher-student relationships and therapist-client relationships, and standardized tools exist to measure the impact of relationship quality in those fields. Despite the importance of relationships in child life, no evaluative measure exists to understand and systematically define the quality of relationships between CCLS and the children they serve. A tool of this type would allow the profession to demonstrate how positive relationships promote better outcomes for patients. The current study aims to address this gap by adapting existing scales measuring adult-child relationships to measure the CCLS-patient relationship.
Measures of Adult-Child Relationships
Children’s outcomes can be influenced by the quality of the relationships they have with adults throughout their childhood, such as their relationship with their parents, teachers, and therapists. Although the parent-child relationship is arguably the most influential relationship for children (Nievar et al., 2014; Pianta et al., 1997), teachers also play an instrumental role in their students’ development. The quality of student-teacher relationships has consistently been linked to children’s social, emotional, and academic development (Birch & Ladd, 1997; Garner & Waajid, 2008; Hamre & Pianta, 2001). Similarly, for children in therapy, positive child-therapist relationships have been associated with greater therapeutic changes and fewer barriers in treatment (Kazdin et al., 2005; Shirk & Karver, 2003). Given that CCLS-patient relationships resemble other non-parental adult-child relationships, it would be reasonable to expect that the quality of the relationship a CCLS has with their patients is also related to children’s psychological, physical, and emotional outcomes during hospitalization and possibly long term. The first step in examining these proposed associations is establishing a reliable and valid measure of CCLS-patient relationship quality.
Existing measures of adult–child relationships can be adapted for this purpose. By adapting validated measures rather than creating a new tool, we leverage their established reliability and validity while tailoring items to the CCLS–patient context, thereby enhancing both scientific rigor and comparability with prior research. For example, the Student-Teacher Relationship Scale (STRS) is a widely validated tool used to measure the teacher’s perceived closeness, conflict, and dependency with their student (Pianta, 2001). A close teacher-child relationship is characterized by warmth, support, and openness, whereas conflictual relationships consist of frustration and perception of difficulties with a particular child. Dependency describes relationships in which the teacher perceives the child as being overly reliant on the teacher. These characteristics of closeness, conflict, and dependency may align with the experiences of CCLS whose relationships with patients require empathetic concern, clear communication, and establishing professional boundaries (Boles et al., 2020). Additionally, some aspects of child life practice, such as providing education about diagnoses and procedures and offering support over repeated encounters, resemble how teachers engage with students, suggesting that a measure of teacher-student relationships has potential to be adapted to measure CCLS-patient relationship quality.
However, child life services differ in important ways from classroom education as relationships with patients are developed in the context of highly stressful situations and are focused on addressing individualized therapeutic goals (McCue, 2018). This suggests CCLS-patient relationships may more closely resemble those developed between therapists and clients. The Agnew Relationship Measure (ARM) is a validated measure used to evaluate the quality of bond, partnership, confidence, openness, and client initiative within therapist-client relationships (Agnew-Davies et al., 1998). Agnew-Davies and colleagues (1998) define bond asprovision of support and understanding from the therapist, whereas partnership is the effort in care shared by the therapist and their client. Confidence reflects the therapist’s view of how confident the client is in the therapist’s skill and competency. Openness is the client’s ability to express their thoughts and concerns without restraint, and client initiative measures the therapist’s perception of the client taking the lead in their care. Assessing a sense of trust and patient engagement through these scales may better assess the quality of CCLS-patient relationships.
Present Study
The goal of the present study was to identify a measure that can accurately assess the quality of the relationship between a child life specialist and their patient. Established measures used to assess teacher-student or therapist-client relationships could potentially be employed, but it is not known which scale is more applicable for measuring the CCLS-patient relationships or whether the scales would measure the CCLS-patient relationships reliably and validly. In this study, CCLS were provided the opportunity to complete two existing measures (STRS and ARM) assessing their relationship with a specific patient and to provide feedback regarding their experience. Two research questions were explored. First, which scale do CCLS perceive to be more applicable to their relationships with patients? We hypothesized that CCLS would view the ARM as more applicable due to the therapeutic nature of CCLS-patient relationships. Second, are these measures reliable and valid when used to assess CCLS-patient relationships? Internal consistency was examined to assess reliability, and construct validity was determined by examining factor structures, meaningful associations between subscales within and across measures, and differentiation of scores based on CCLS and patients’ characteristics.
Methods
Participants
The present study includes responses from 77 Certified Child Life Specialists (CCLS). Though 208 CCLS initiated the survey, 131 responses were not included in analyses due to significant patterns of missing data considered to be Not Missing at Random (NMAR). The final sample consists of 66 complete responses and 11 partially complete responses which had fewer than 10 missing items distributed throughout the survey. The missingness of the data was assessed to compare the demographic characteristics of participants in the final sample to those who did not finish the survey. Analyses determined that those with missing data were characteristically very similar to those who were included in the sample.
As shown in Table 1, respondents were primarily White (n = 74, 96.10%), non-Hispanic (n = 66, 85.70%), females (n = 73, 94.80%), with master’s degrees (n = 54, 70.10%). The CCLS were on average 34.79 years old (SD = 9.88, range = 24-58) with 8.58 years of work experience (SD = 8.26, range = 0.17-34.83). Socioeconomic status (SES) was reported using the MacArthur Scale of Subjective Social Status (Adler et al., 2000). The mean rating of 6.19 (SD = 1.19) indicates respondents perceived their SES to be slightly above average.
Each CCLS reported the demographic characteristics of one patient with whom they had a relationship (n= 77; Table 2). Of these patients, 50.60% were female (n = 39), and the majority were White (n = 46, 59.70%) and non-Hispanic (n = 52, 67.50%). Approximately half of patients were seen in inpatient settings, (n = 39, 50.60%), 27 were seen in outpatient settings (35.10%), and 11 did not fall within either category (14.30%). On average, patients had been under the CCLS care for 12.22 months (SD = 23.35, range = .01-168) and had spent an estimated 74.97 hours with the CCLS (SD = 177.10, range = 1-1344).
Procedure
CCLS were recruited via social media, emails to hospital-based child life departments, and word of mouth to complete an online survey in Qualtrics. Participants provided informed consent and answered the screening question “are you a Certified Child Life Specialist?” CCLS participants provided background information regarding demographic characteristics (e.g., age, gender identity, race, and ethnicity) and professional experience (e.g., how long they’ve been practicing and what department they work in). Participants were asked to think of one patient with whom they had built a relationship within the past three months, preferably a child with whom they have worked for at least one month. Participants answered questions about this patient’s demographic characteristics (e.g., race, ethnicity, sex) and their interaction with the patient (e.g., whether they encountered the patient for inpatient or outpatient services, how long they have known the patient). Then, participants completed two measures to gauge the quality of their relationship with this patient. In addition, they were asked to rate each item from the relationship measures based on how appropriate they believed it to be for measuring CCLS-patient relationships. This project (7831) was approved as exempt by Texas State University IRB.
Measures
Student Teacher Relationship Scale (STRS)
The STRS is a 28-item tool with three subscales used to measure the teacher’s perceived conflict, closeness, and dependency with a student (α=.89; Pianta, 2001). The STRS is scored using a 5-point Likert scale ranging from “strongly disagree” to “strongly agree.” For use in the current study, scoring was adapted to a 7-point scale ranging from “strongly disagree” to “strongly agree” in order to establish consistency across measures. The closeness scale consists of items such as “I share an affectionate, warm relationship with this child” (α=.86). The conflict scale consists of items such as “This child and I always seem to be struggling with each other” (α=.92). The dependency scale consists of items such as “This child appears hurt or embarrassed when I correct him/her” (α=.64). The wording of three items was adapted to align with CCLS-patient interactions (Appendix A). For example, two items from the conflict subscale referenced the child’s reaction to the teacher as a disciplinarian, which is not a role typically fulfilled by a CCLS. In consultation with CCLS on the research team, the wording was adjusted to ask about the child’s association of the CCLS with treatment or pain, which would be a more common source of negative interactions in the CCLS-patient relationship.
Agnew Relationship Measure (ARM)
The ARM is a validated tool used to evaluate the quality of therapist-patient relationships (Agnew-Davies et al., 1998). Though designed for adults, the ARM was selected because the therapist self-report measure does not require child or parent report for analysis. The 28-item scale utilizes a 7-point Likert scale ranging from “strongly disagree” to “strongly agree” and consists of five subscales. Bond consists of items such as “My client feels free to express the things that worry him/her” (α=.85). Partnership consists of items such as “My client and I are willing to work hard together” (α=.81) Confidence consists of items such as “I feel confident in myself and my techniques” (α-.86). Openness consists of items such as “My client feels that she/he can openly express her/his thoughts and feelings to me” (α=.86). Client initiative consists of items such as “My client takes the lead when she/he is with me” (α=.55). Across all items, the word “client” was changed to patient, and the wording of several items was adapted to be appropriate for working with children or to provide additional clarity of what was being asked. Specific item-level changes are outlined in Appendix A.
Applicability of Scale to Child Life
For each item of the STRS and the ARM, participants rated how applicable the item was to their relationships with patients. Responses for each item were given using a 5-point Likert scale ranging from “definitely does not apply” to “definitely applies.” A mean rating of applicability for each measure was calculated to determine the perceived relevance and clarity of the items in a clinical context
Data Analysis
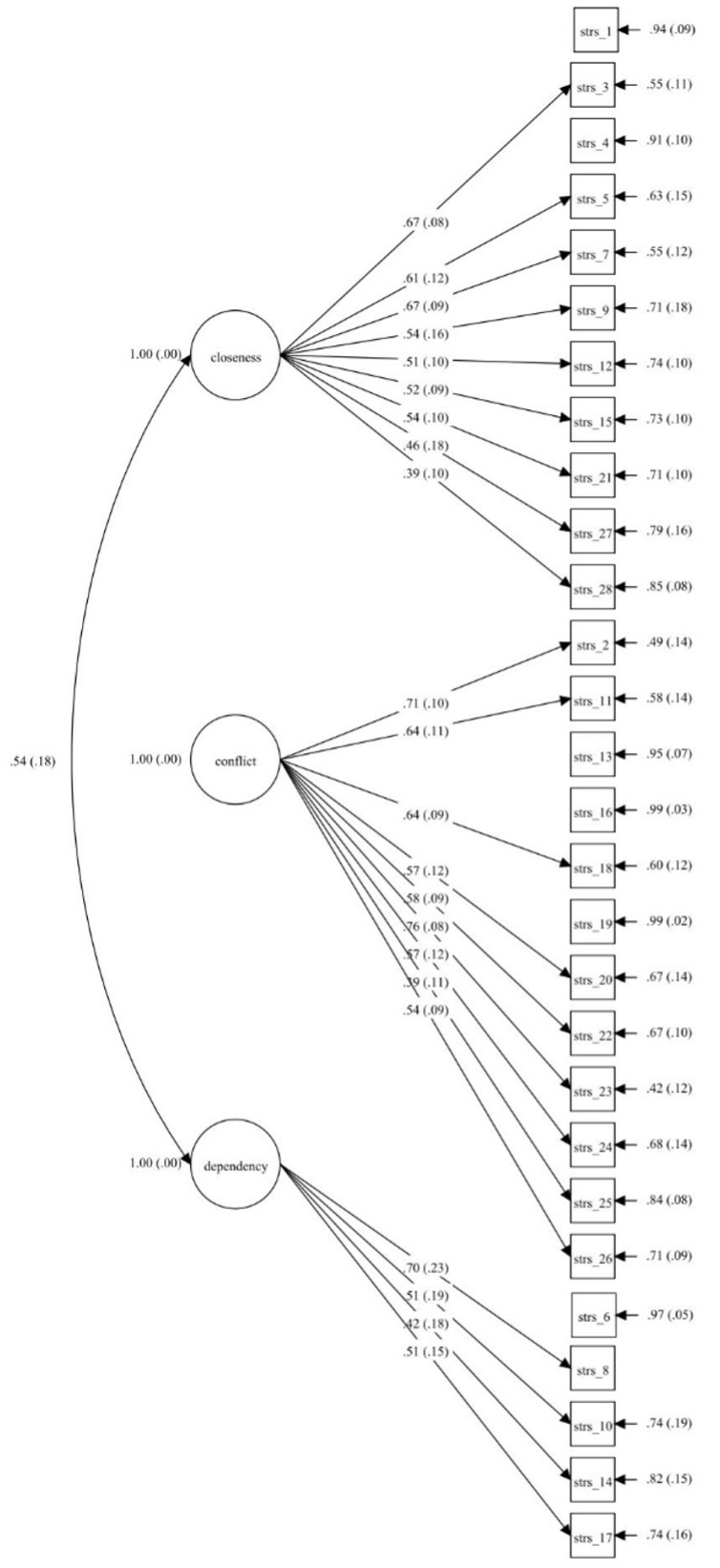
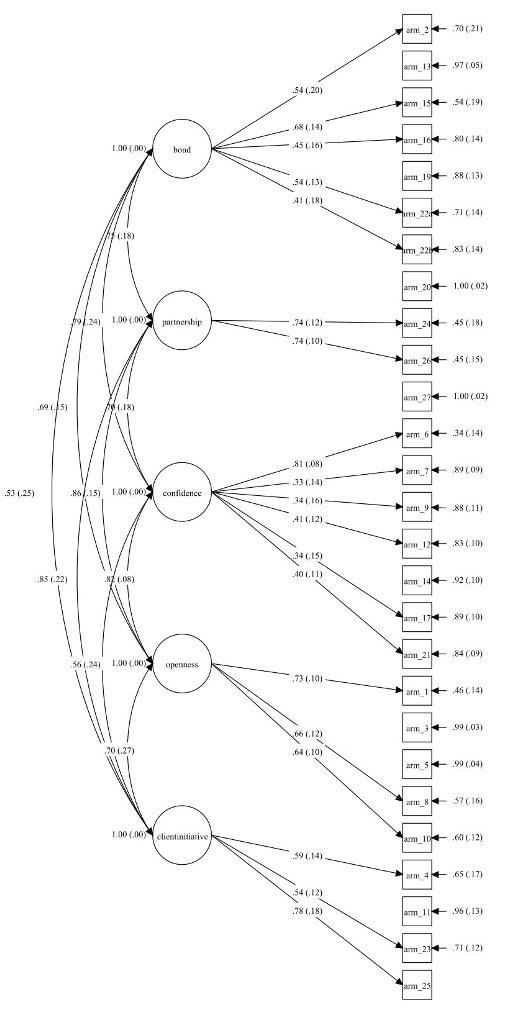
Initial data analysis was conducted in SPSS version 27 (IBM Corp., 2020). Preliminary analyses included descriptive statistics of study variables. To address the first research question, applicability ratings for the STRS and ARM were compared using a paired samples t-test with an alpha of .05. To examine the second research question, confirmatory factor analyses (CFA) were conducted separately for the STRS and the ARM in Mplus version 7 (Muthén & Muthén, 2012). All models were estimated using a Full Information Maximum Likelihood (FIML) estimator for the full sample (N = 77), addressing both missing and nonnormally distributed data. For the STRS, three factors were specified based on the original factor structure of closeness, conflict, and dependency. For the ARM, five factors were specified based on the original factor structure of bond, partnership, confidence, openness, and client initiative. The following fit statistics and thresholds were used Kline, 2015): Model Chi-Square (X2; p > .05), Comparative Fit Index (CFI ≥ .90), Tucker Lewis Index (TLI ≥ .95), Root Mean Square Error of Approximation (RMESA < .08), and Standardized Root Mean Square Residual (SRMR < .08). Cronbach’s alpha was calculated to examine internal consistency of the subscales, and correlations examined relations between the subscales within and across the measures to shed light on construct validity. Finally, correlations, t-tests, and one-way ANOVAs were utilized to determine whether the scores differed based on CCLS and patient characteristics.
Results
Item-level ratings of applicability were averaged across all items for each scale, resulting in a mean applicability score of 3.59 (SD = .63; range = 2.29-5.0) for the STRS was and a mean applicability score of 3.77 (SD = .57; range = 2.22-5.0) for the ARM. Paired samples t-test revealed a statistically significant difference between average applicability ratings across measures, demonstrating that CCLS rated the ARM as more applicable to their relationships with patient compared to the STRS, t(76) = -4.22, p < .001.
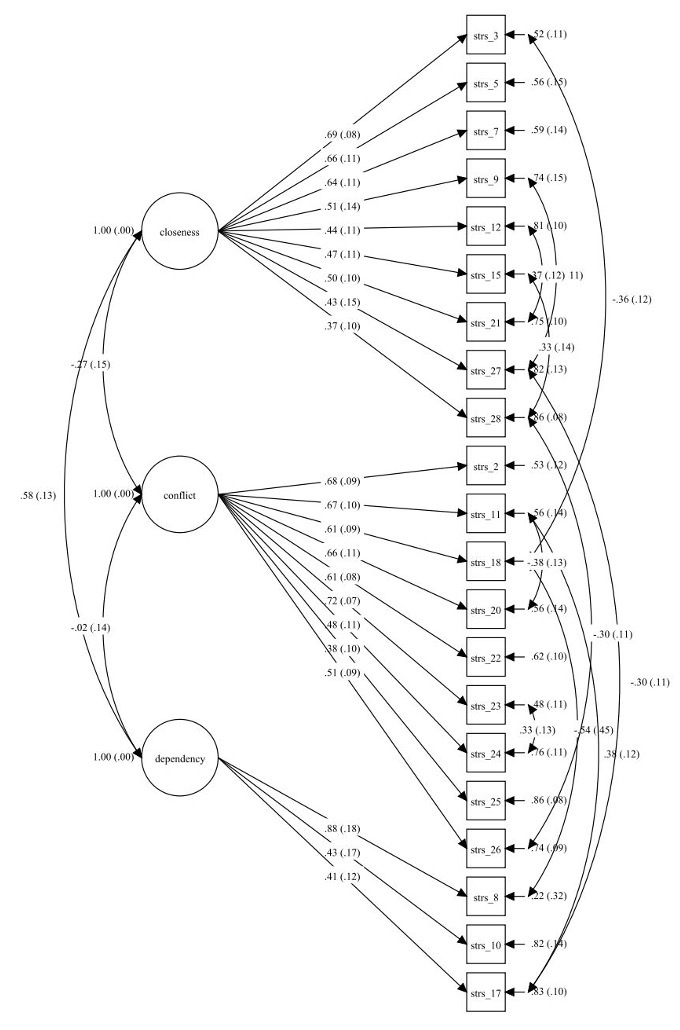
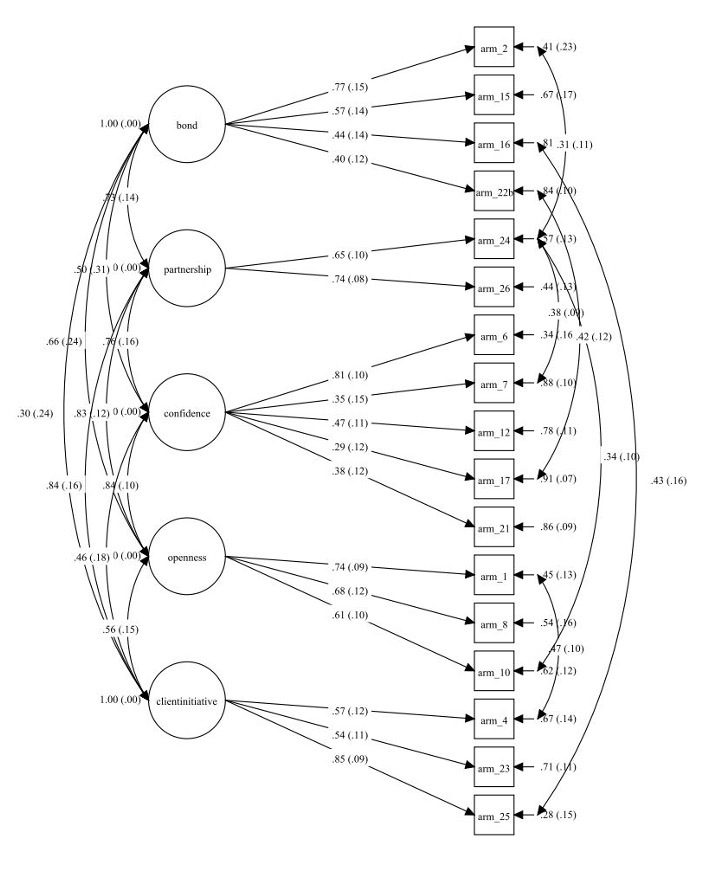
Confirmatory factor analysis (CFA) revealed that the initial models for the STRS and the ARM did not meet thresholds for adequate fit (Appendix B, Figures 1 and 2). Modification indices of the initial CFAs were examined to adapt the measures for CCLS-patient relationships. For the STRS, six of 28 items did not load on their assigned constructs and were dropped from the subscales. For the ARM, eight of 28 items did not load on their assigned constructs and were dropped from the subscales. After omitting items that did not load properly and including residual correlations based on modification indices, both models met thresholds for adequate fit and retained the subscales of the original measures (Appendix B, Figures 3 and 4). The statistics of the original and adapted models are described in Table 2. Most subscales showed adequate reliability (α = .63-.84) following adaptation, though the subscales of bond (α =.56), dependency (α =.58) and confidence (α=.55); remained low (see Table 4).
Correlations between subscales across the STRS and ARM were examined for construct validity (Table 5). Significant positive associations were found among closeness, bond, partnership, confidence, and openness, all constructs associated with positive relationship quality. Similarly, conflict was negatively associated with closeness, bond, partnership and confidence. Perception of client initiative was related to partnership, openness, and closeness; bond was associated with dependency.
Analyses revealed scores on relationships subscales differed by CCLS and patient characteristics. On average, CCLS reported that male patients took more initiative in their care than female patients, t(69.64) = 2.66, p = .01). In addition, dependency differed based on SES of the CCLS, F(6,70) = 3.37, p = .01, where CCLS who self-reported lower SES rated their patient higher on the dependency subscale than those who reported a higher SES. Moreover, CCLS years of work experience was significantly correlated with the bond subscale, r = -.26, p = .02, indicating that those who had been working fewer years reported a closer bond with the patient. Finally, CCLS age was significantly correlated with closeness, r = -.24, p = .04, and bond, r = -.29, p = .01, suggesting that younger CCLS reported higher levels of closeness and bond with patients.
Discussion
The purpose of the current study was to examine the use of existing adult-child relationship measures to assess the quality of CCLS-patient relationships. The ARM, a measure of therapist-client relationships, was rated by the CCLS as significantly more applicable than the STRS, a measure of teacher-student relationships. It was unsurprising that the CCLS in the present sample preferred a relationship measure that emphasizes the therapeutic nature of the CCLS-patient relationship. While CCLS do take on the role of teacher when educating patients on diagnoses and procedures, this represents only one type of intervention they may provide. Additionally, while teachers typically navigate relationships with multiple students simultaneously in a group setting, therapists more commonly develop relationships through individualized, supportive interactions, which more closely resembles the dynamics of a CCLS-patient relationship.
Statistical models based on the original STRS and ARM measures did not fit the CCLS-reported data well, whereas adapted models which dropped poorly-loading items fit the data better. Examination of dropped items suggests several possible variables that may have impacted the factor structure of the present data, particularly the important role parents and families play in a pediatric patient’s care. Child life services follow a patient- and family-centered care model (Boles et al., 2020; Romito et al., 2021), and parents are integrated into child life care plans in a way that they may not be with teachers and therapists. CCLS often work in conjunction with parents and less commonly take on the role of primary caregiver, as a teacher does during the school day. Due to the level of family involvement, some items on the STRS and the ARM may not apply to CCLS relationships with patients. For example, the STRS item “This child is uncomfortable with physical affection or touch from me” (reverse-scored) did not correlate with other items in the closeness subscale. Similarly, the ARM item “My patient looks to me for solution to his/her problems” did not correlate with other items on the client initiative subscale. This pattern aligns with evidence that parents typically remain the primary source of guidance and problem-solving support for children and adolescents in healthcare contexts, even as other professionals play complementary roles (Badour et al., 2023). For example, the items “This child appears hurt or embarrassed when I correct him/her” and “If upset, the child will seek comfort from me” received low applicability ratings, likely because parents rather than CCLS fill these roles. Adapted models of ARM and STRS where problematic items were dropped fit the data better than the original models.
Other items from the original measures may not have applied well to the context of child life practice with pediatric patients. For example, the STRS item “This child feels that I treat him unfairly” did not correlate with other items on the conflict scale, perhaps because patients are typically less aware of the relationships CCLS have with other patients compared to a student’s awareness of how the teacher interacts with their classmates. On the ARM, the dropped items “my patient is worried about embarrassing her/himself with me” and “my patient keeps some important things to her/himself, not sharing them with me” were not significantly correlated with other items on the openness subscale. These items are meant to assess whether an adult therapy client is being “closed off” rather than open, but children may demonstrate reluctance to engage openly with the CCLS through different behaviors.
Although several items were dropped from the STRS and ARM based on CFA results, the adapted versions retained the core subscales and constructs of the original measures, suggesting that the reduced scales still capture the central dimensions of relationship quality (e.g., closeness, conflict, bond, partnership). Importantly, the items removed appeared to reflect contextual differences between the roles of teachers, therapists, and CCLS rather than a loss of theoretically essential content. Thus, the adapted measures maintain practical and theoretical meaning for assessing CCLS–patient relationship quality, while also increasing contextual relevance to child life practice. Furthermore, the correlations between subscales indicate construct validity, suggesting both the STRS and ARM are capturing similar aspects of high-quality adult-child relationships.
Associations among subscales also provide valuable insights regarding the constructs that contribute to CCLS-patient relationship quality. It was notable that CCLS perception of the patient’s initiative was related to closeness, openness, and partnership. Much of child life practice emphasizes the importance of child-led interventions and encourages patients to advocate for themselves and implement coping skills independently (Humphreys & LeBlanc, 2016). Interestingly, perception of child dependency was positively associated with closeness but negatively associated with the ARM subscales of bond and partnership. This suggests that asking CCLS to consider patient initiative in the relationship may be a more appropriate indicator of relationship quality than attempting to measure patient dependency.
Analysis of demographic characteristics and relationship measures revealed a number of significant differences. CCLS reported that male patients took more initiative in their care than female patients. It is possible that gender biases related to expectations for assertiveness and emotional expression affected CCLS perception of “initiative.” Additionally, dependency CCLS who reported lower SES rated patients as more dependent on them. CCLS who perceive themselves as having a lower SES in comparison to other professionals may also feel their work is undervalued or not adequately compensated, feelings that contribute to burnout (Hoelscher & Ravert, 2021). This may result in a more negative perception of the emotional involvement demanded by some patients. Given that dependency was also correlated with closeness, however, further research is needed to better understand these relations.
Reports of patient relationship quality also varied by the age and professional experience of the CCLS. In this sample, older CCLS tended to report lower levels of closeness and bond with patients than younger CCLS. Additionally, CCLS who reported more years of work experience tended to report weaker bonds with patients. These associations are correlational and should not be interpreted as predictive or causal. Some literature suggests that emotional distance and detachment have been valued by nurses to reduce emotional distress when working with pediatric patients (Rollins et al., 2018). Older and more experienced CCLS may intentionally create more emotional distance when building relationships with patients to reduce burnout. It is also possible that more experienced CCLS hold additional responsibilities, such as student or staff supervision, that may limit the amount of time spent developing close patient relationships. CCLS who reported spending more time with their patients reported a closer bond with them, and this correlation remained significant for CCLS working with inpatient or outpatient populations. This suggests that the amount of time spent with a patient has an important influence on the quality of the CCLS-patient relationship which may outweigh other factors.
Limitations and Future Directions
Our sample size in the present study was small, resulting in a reduction of power. The length of the survey and lack of incentive likely contributed to the number of surveys that were initiated but remained incomplete. Given the relatively small sample size (N = 77), the CFA results should be interpreted with caution, as smaller samples may limit model stability and generalizability. Future research with larger samples or complementary approaches such as exploratory factor analysis and test–retest reliability is warranted to strengthen validation.
To ensure patient privacy, age and diagnosis information were not collected from CCLS, limiting our ability to explore how relationship quality may relate to the patient’s developmental level or medical status. Exploratory analyses showed differences in some relationship ratings by patient sex, though it is possible these were influenced by gendered expectations (e.g., female children are more passive whereas male children should take initiative). Given that CCLS work with a wide range of ages and diagnoses and diverse populations, future work should include examination of patient characteristics and how these may interact with CCLS characteristics and beliefs to influence relationship quality.
Based on CCLS ratings and examination of statistical model, we recommend the adapted ARM scale would be most appropriate to pilot for future studies of CCLS-patient relationships. While the applicability ratings provided useful feedback on the perceived relevance of the ARM scale, they were not intended to serve as evidence of psychometric validity. Rather, this process served as an initial step in measure refinement; future research should employ more rigorous validation methods, such as convergent validity testing, to formally establish the ARM measure’s validity. Future research with a larger sample size is also needed to further adapt the model; for example, the family-centered care aspect of child life services was not adequately captured by either scale. Furthermore, studies that measure patient outcomes will provide insight into how CCLS leverage relationships to support children’s coping and well-being, and future measurement work should include consideration of the influence of parents and families on CCLS-patient relationships. Collectively, these steps are essential to complete before this measure can be used as an accepted tool for assessing CCLS–patient relationships in practice or research.
Implications for Practice
Research in education and psychotherapy shows that the quality of adult-child relationships has important implications for child outcomes. The child life profession currently lacks a standardized tool to measure CCLS-patient relationships and evaluate the intangible ways CCLS support child well-being. Identifying, adapting, or creating a tool to reliably measure these relationships is an important next step as the child life field strives to implement research-backed, evidenced-based services for patients and families. The adapted ARM scale represents an initial effort toward this goal; while it is intended primarily for research at this stage, it may eventually support professional reflection by helping CCLS examine relationship patterns across patients and identify potential biases. The ability to identify the specific constructs and behaviors of high-quality CCLS-patient relationships will support professional development, validate the impact of child life services on patient experience, and enhance positive outcomes for patients and families.
.jpg)
.jpg)
_model.jpg)
_model.jpg)