Play is an essential, distinguishing characteristic of child life work (Boles et al., 2020; Romito et al., 2021), leveraged as a tool to both support children’s development and to identify and address areas of concern. However, perspectives on play are more complex than they may initially appear on the surface. The education and training child life specialists receive tends to espouse a nondirective child-centered view of play, though in practice play is often applied in directive ways to teach, prepare, distract, and address specific therapeutic goals (Thompson, 2018). This suggests a theoretical divide between a clinical approach that is more play-based and one that is more focused on preparation and education, yet such a dichotomy obscures the many ways play can operate within child life practice. This article examines theory and research on adult involvement in play, highlighting the spectrum of guided play approaches that exist between nondirective and directive play. Then, based on seminal work from child life pioneer Rosemary Bolig, a revised and expanded continuum of play in child life practice is described. This continuum can serve as a guide for emerging professionals to intentionally employ play in ways that support the various needs of children and families.
Theoretical Views on Play and Adult Involvement
Fundamental differences exist in how children’s play is viewed in the classical developmental theories upon which child life training and practice are based. Piaget proposed that play supports children in actively exploring the world to construct knowledge; through play interactions, whether with physical objects or in games with peers, children engage in assimilating and accommodating their mental schema to reality (Piaget, 1962; Piaget & Campbell, 1977). From this view, play functions to support cognitive development and understanding, and children benefit most from directing their own play with minimal adult involvement. The psychoanalytic perspective proposes a different purpose for play but arrives at a similar conclusion that play should be child-directed. Erikson (1950), whose theory of psychosocial development was grounded in years of clinical practice as a psychoanalyst, argued that children will choose to play in ways that resolve internal conflicts, providing a sense of mastery and control. Play therapy is grounded in this belief that self-directed play helps children process distressing or stressful experiences (Axline, 1969; Landreth, 2012). Given that both Piaget and Erikson viewed child self-direction in play as paramount, neither theorist assigns an explicit role to adults to initiate or direct how children play to achieve a specific goal.
In contrast, sociocultural theory suggests adult involvement has an important role in children’s play. Vygotsky (1978) explicitly viewed play as a zone of proximal development in which children can begin to engage in skills that are beyond their ability to enact without support. Though children are able to make choices during play, they must also navigate explicit and implicit rules, which are learned through interaction with adults and peers (Van Oers, 2013; Wood, 2014). The involvement of adults or older peers is viewed as essential for helping young children to develop the type of mature, imaginative play that supports development of cognitive and socioemotional skills (Bodrova & Leong, 2015). From this perspective, adult involvement in play can facilitate children’s engagement and scaffold learning.
Despite the limitations of these theories (Koller & Wheelwright, 2020), such classical developmental paradigms remain a primary influence on child life education and practice, particularly where the topic of play is concerned. These perspectives seem to establish a dichotomy, separating play that is child-centered and supports individual development and well-being from play that includes adult direction and guidance, often to facilitate socially desirable goals. This divide between child-driven and adult-directed play is echoed within the child life field. Though child life scholars acknowledge that play activities may be structured and guided by the child life specialist to promote specific therapeutic goals (Burns-Nader & Hernandez-Reif, 2016; DelPo & Frick, 1988; Koller, 2009), the Official Documents of the Association of Child Life Professionals explicitly promote a child-centered play paradigm. For instance, the child life competency related to play refers to “child-centered responses,” “child-directed play skills,” and the establishment of play spaces that “encourage children to choose and explore at their own pace” (Association of Child Life Professionals, 2019, p. 2). Yet, a survey of play in child life programs across North America found that adult-directed play – used for teaching, preparation, and distraction – was being used more widely than child-centered play (Vilas, 2014). This shifting emphasis is also reflected in research on child life interventions; a review of child life studies from 1998-2017 found a significant decrease in the number of studies focused on play compared to those on preparation and procedural support, more adult-directed interventions (Boles et al., 2021). These discrepancies suggest an urgent need to re-examine how play theories inform child life practice and to consider what can be done to bridge this gap.
Play in Child Life Practice
Nearly 40 years ago, child life scholar Rosemary Bolig and her colleagues described a cognitive-affective approach to child life programming that sought to unify theoretical perspectives (Bolig et al., 1986; Bolig & Gnezda, 1984). The proposed model initially outlined four roles that child life specialists can fulfill to support the hospitalized child in returning to baseline play behavior, ranging from more to less directive. The child life specialist’s underlying goal was always framed as supporting the child’s autonomy and opportunities for unstructured play, but Bolig and colleagues (1986) recognized that some hospitalized or traumatized children may only be able to engage in play with a high level of adult guidance. At the more directive end of the continuum, the child life specialist provides highly structured, sometimes repetitive play to help build trust and a sense of predictability (Bolig & Gnezda, 1984). As an “environmental organizer,” the child life specialist provides limited choices and uses modeling to reinforce and extend the child’s attempts to engage in play. Control over play shifts to the child when the child life specialist acts as a “conceptual organizer” who continues to reinforce, encourage, and extend the child’s play ideas. In the least directive role, the child life specialist assesses the child’s ongoing play and only selectively engages to facilitate emotional processing. As children adjust to the hospital setting, the adult’s role is expected to shift from more to less directive, though child life specialists must continually reassess and flexibly adjust their approach based on the individual child’s needs (Bolig et al., 1986).
A streamlined version of this play continuum is provided in one of the foundational texts required for child life certification, Meeting Children’s Psychosocial Needs Across the Health Care Continuum (Rollins et al., 2018). Referred to as the “play to not play” continuum, it spans from nondirected play through guided play to directed “not play” activities (Bolig, 2018), focusing more generally on the amount of adult direction rather than the more detailed description of roles previously described. Notably, Bolig warns of the negative consequences of adult over-involvement in play, stating “more active or directive roles have certain dangers; there is a subtle but critical line beyond which adults can turn children’s play into ‘not play’” (Bolig, 2018, p. 102). This is a significant shift from the earlier view that adult guidance may be needed to support the play of hospitalized children (Bolig et al., 1986), and it may be the result of Bolig’s growing concerns that child life specialists increasingly emphasized adult-directed activities, such as preparation, over child-directed play (Bolig et al., 1991). As noted above, this shift away from child-directed play to adult-directed intervention remains evident in clinical practice (Vilas, 2014) and research focus (Boles et al., 2021).
This leaves students and professionals caught between two perspectives. Child life official documents and textbooks tend to encourage a child-centered view of play, whereas clinical training and research focus on utilizing adult-guided or directed play to achieve specific therapeutic goals. Further, opportunities for emerging professionals to learn how to facilitate play in clinical environments may be limited when child life programs must respond to policy and staffing changes, as was observed during the COVID-19 pandemic when volunteer opportunities and playroom access were restricted (Jenkins et al., 2023). Similar challenges have been encountered in the education field, as practitioners and experts seek to integrate play in meaningful ways to support learning both inside and outside classroom environments while navigating administrative and policy demands. Examining how scholars have conceptualized different approaches to play and adult involvement in the context of learning provides insight into how this apparent tension between child-centered and adult-directed play may be resolved.
Play on a Spectrum: Lessons from Playful Learning
Within the literature on playful learning, researchers have also described play as a spectrum with varying levels of adult support (Pyle & Danniels, 2017; Zosh et al., 2018). Similar to the continuum described in Bolig’s work (Bolig, 2018; Bolig & Gnezda, 1984), child-directed free play on one end is contrasted with adult-directed activities on the other. The extreme end of adult involvement is no longer considered play at all and is labeled direct instruction (Weisberg et al., 2013; Zosh et al., 2018), similar to Bolig’s (2018) view that adult involvement at some point shifts an activity to “not play.” Between these extremes, however, education scholars have defined guided play as a “middle ground” that integrates child autonomy with adult scaffolding (Weisberg et al., 2016). Bolig’s (2018) most recent conceptualization also includes guided play, indicating this construct is meaningful within child life practice as well as education. Three key factors, described below, provide additional nuance for understanding how adults engage in guiding children’s play.
Given that play is often construed as voluntary and intrinsically motivated (Gray, 2017), there seems to be an inevitable tension in suggesting that any amount of adult guidance can produce “true play” (Brown, 2007, p. 27). However, proponents of guided play argue that the critical element is the child’s level of autonomuy. Designed and initiated by the adult, guided play may appear less voluntary in comparison to free play, yet, unlike direct instruction, the child can freely decide the direction of the activity (Zosh et al., 2018). Guided play maintains its playful nature because the child retains control and remains active and intrinsically motivated (Weisberg et al., 2013). The primary role of the adult in guided play is to structure the play situation. According to Weisberg and colleagues (2016), guided play is like “mise en place” within a chef’s kitchen; the adult ensures the materials, resources, and time are appropriate and available to facilitate children’s engagement and promote their natural desire to learn. Adults may use questions and comments during guided play to direct children’s attention toward learning goals, but a key factor of guided play is maintaining children’s autonomy and intrinsic motivation.
An additional factor that needs to be considered is the extent to which the adult engages in making purposeful and targeted decisions about when and how to provide guidance to the child. Guided play is only considered play because the child can exercise control over how the activity proceeds; when the adult exerts too much direction over the activity, it skews from play to instruction (Zosh et al., 2018). This concern that too much adult involvement undermines the innate benefits of children’s play is evident among educators who use play in their classrooms. In a qualitative study of kindergarten teachers, a subset of participants felt teacher involvement in play inherently shifted the locus of control away from the child, essentially “hijacking play” (Pyle & Danniels, 2017, p. 274). However, other teachers emphasized being intentional about the type of support they provided for children’s play and maintaining a balance between adult structure and child autonomy. Responsive adult interactions that are a “good fit” for the child’s needs – meaning teachers provided more direct play guidance for children in need of more support and minimal guidance to children who needed less support – were found most effective for extending children’s play to support learning and development (Trawick-Smith & Dziurgot, 2011). Thus, it is the individualized assessment of the child’s needs in the moment that influences how the adult responds and how much guidance is provided.
Even within the guided play literature, there are different views regarding whether adults should engage in play as co-participants or provide prompts for play through suggestions and comments. Some view the adult role as scaffolding from outside the play (Weisberg et al., 2016) whereas teachers in classrooms often engage in collaborative play alongside children (Pyle & Danniels, 2017). Enz and Christie (1997) proposed a continuum of teacher play interaction styles based on observations in a preschool classroom. Three of these roles, all of which reflect guided play approaches, seemed to enhance the quality of children’s pretend play. The “stage manager” remains outside the play but provides materials, responds to children’s requests, and makes comments or minor suggestions. In the “co-player” role, the adult joins the pretend play in a minor role and subtly scaffolds the play, whereas adults who enact the “play leader” role are more active participants, interjecting new ideas and plot complications but still following children’s ideas and actions. Of note, these roles are also described in Bolig’s (2018) chapter on play in healthcare settings, with an emphasis on selecting roles with sensitivity to children’s individual needs and reactions.
Thus, a third important factor in determining how much adult guidance is appropriate in play is the adult’s goal for the child, based on an assessment of the child’s needs and abilities. The view in child-centered play therapy is that adults should participate in play only at the invitation and continued direction of the child, based on the over-arching goal to allow the child to play in whichever way they need (Axline, 1969; Landreth, 2012). In contrast, educators have argued that adults who position themselves inside the child’s play frame gain important opportunities to extend the child’s thinking and create a zone of proximal development (Devi et al., 2021; Fleer, 2015). Not only are these differing perspectives on adult involvement in play clearly grounded in distinct theoretical perspectives, but they also emphasize different goals. Play therapy goals focus on emotional expression, autonomy, mastery, and building a therapeutic relationship. Education goals focus on learning specific content as well as supporting the development of cognitive and socioemotional skills. Child life specialists may focus on any of these goals, and therefore it is necessary to consider how their involvement in play supports the specific goal they have for the child at that moment.
In sum, keeping these three factors in mind – respect for child autonomy, sensitive and intentional adult interaction, and focus on a specific goal – may be especially useful for child life specialists as they make decisions regarding how much guidance and direction to offer in play interactions. In the next section, these factors are integrated into discussion of a revised and expanded continuum of play in child life, grounded in Rosemary Bolig’s foundational work.
An Expanded Continuum of Play in Child Life Practice
The three characteristics of adult involvement identified provide a framework for understanding the spectrum of roles child life specialists can take in children’s play. Child life specialists provide play opportunities for many different purposes, and the amount of direction and structure provided depends on assessment of the child (Burns-Nader & Hernandez-Reif, 2016; DelPo & Frick, 1988). As exemplified in Bolig’s original model (Bolig et al., 1986; Bolig & Gnezda, 1984), adult involvement occurs along a continuum, and the same activity might be used with varying levels of adult involvement. Though therapeutic and medical play are often adult-structured to a degree, these activities can include a high degree of child autonomy and minimal adult direction during the play itself (Brown, 2007; DelPo & Frick, 1988). Conversely, normative play may be highly directive if a child is withdrawn or extremely ill and unable to sustain independent play (Bolig et al., 1986). Thus, it is not the type of play which determines the appropriate amount of adult involvement; rather, it is the child life specialist’s assessment of the child’s current needs and planned goals for intervention that should guide their engagement in the child’s play.
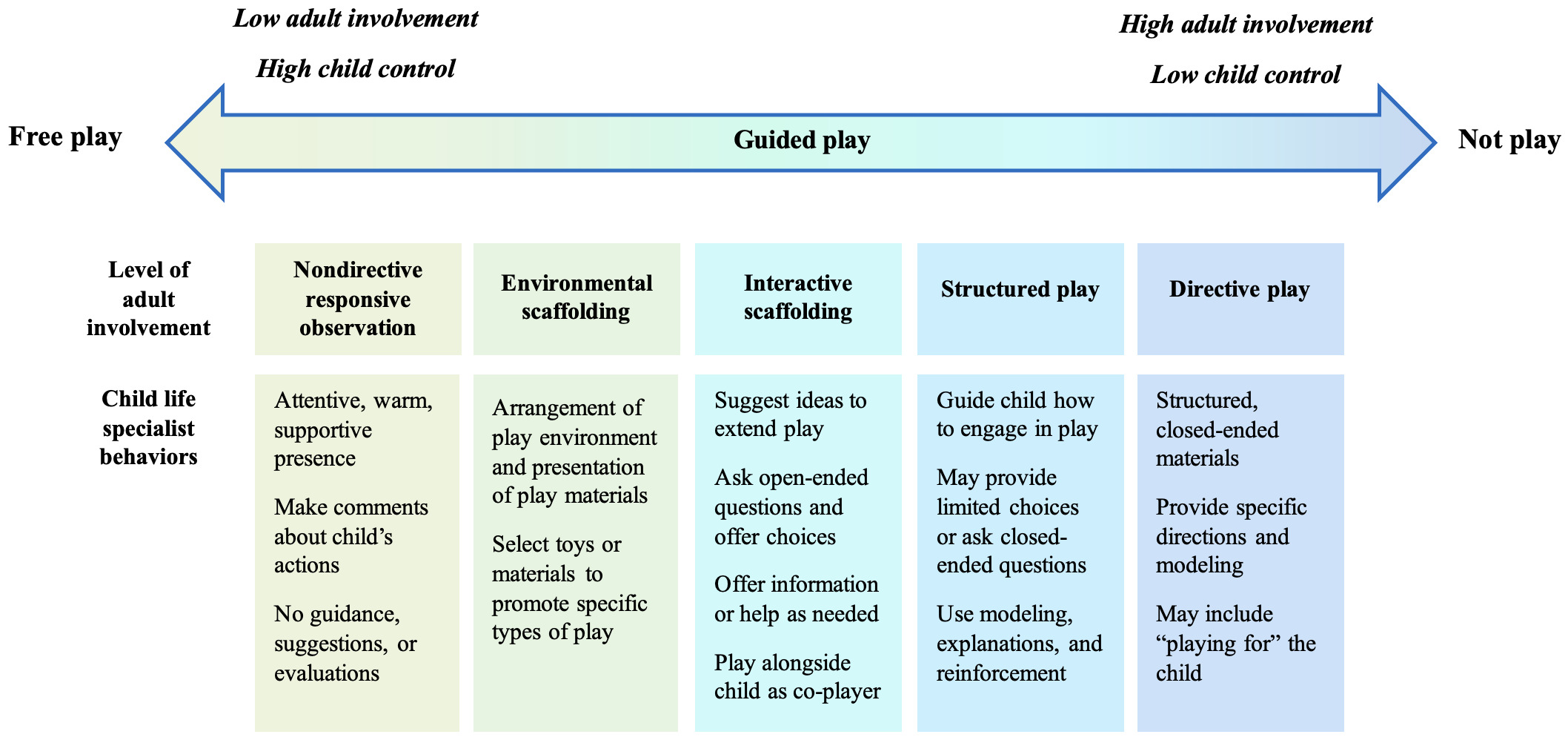
An expanded continuum of adult involvement in play is proposed in Figure 1. Like the previously described continuums, it spans from free play to adult-directed “not play” activities and includes the key dimensions of child control and adult direction. However, the focus is on the degree of child control and adult involvement, acknowledging the existence of multiple incrementally more directive approaches to adult guidance in line with literature in education (Pyle & Danniels, 2017; Trawick-Smith & Dziurgot, 2011) and child life practice (Bolig et al., 1986). Guidance regarding what adult involvement looks like at each point on the continuum is provided within the figure as a quick reference; more detailed description of how this applies to child life practice is provided below along with hypothetical case examples.

Nondirective Responsive Observation
Immediately beside child-directed free play on the continuum, the role of nondirective, responsive observer includes being present and attentive during a child’s play without providing guidance, suggestions, or evaluative comments. This role mirrors the type of adult involvement recommended in child-centered play therapy (Axline, 1969; Landreth, 2012). Providing a warm, nondirective presence during play helps normalize unfamiliar environments and establish a sense of safety that facilitates child-directed play. Child life specialists may enact this role to assess development and coping as a child plays independently or with peers in a playroom, camp, or support group setting. Nondirective but responsive observation is also an effective way to engage in rapport building with a patient who may be wary or shy, as the child life specialist communicates verbal and non-verbal interest in the child’s activity but does not actively attempt to engage in their play or physically touch the child’s toys or materials.
Case example. Aiden is a 2-year-old being seen in the outpatient clinic for the first time, and his chart indicates a possible developmental delay. Aiden is sitting on the floor playing with several toy cars when the child life specialist enters the room. Aiden watches warily as the child life specialist introduces services to his parents. The child life specialist sits on a low stool a few feet away, saying, “I’ll sit over here so you have lots of room to play.” Aiden begins to place the cars in a line, carefully ensuring that each car is oriented in the same direction. The child life specialist comments, “You’re making sure they are all lined up.” Aiden begins to roll one car back and forth over the tile as the wheels make a sound, and the child life specialist narrates his actions, “You’re checking how that one moves. It’s making a sound on this floor.” Aiden gives the car a sudden push, sending it rolling across the room, and shouts with excitement as it hits the wall. The child life specialist comments, “You made that car move really fast. It was fun seeing it run into the wall.”
Environmental Scaffolding
Environmental scaffolding focuses on organizing the play environment or situation to prompt opportunities for children to play in certain ways. Environmental scaffolding fits within the construct of guided play (Weisberg et al., 2016) but represents a more indirect role in which child life specialists subtly shape what children play rather than directly guide how they play. This may occur through the selection and set-up of a play environment, such as the choice of playroom materials or how an activity is visually presented, or through the child life specialist’s intentional selection of specific toys or activities that correspond with a child’s assessed needs. Examples might include storing medical play items, like a toy syringe, near the play kitchen in a playroom that serves patients with diabetes or providing board books and blocks to the parent of an infant to promote developmentally supportive parent-child interaction.
Case example. The child life program is hosting a medical play clinic at a community health resources event. One table consists of blank cloth dolls, markers, and doll-sized gowns, and the other table is covered with a variety of real and pretend medical equipment and supplies. Knowing that the public health department is offering seasonal vaccinations during the event, alcohol wipes, plastic syringes, and band-aids are provided among the medical supplies. When families arrive, child life staff briefly explain that children can create a “patient” to take care of with any of the medical items they see. Most children decide to make a patient doll first, though some go directly to the medical play supplies and begin to play on their own stuffed animals. Several children are immediately drawn to the syringes and begin giving “shots” to their dolls while other children role play giving their doll a “check up” using the pretend play toys.
Interactive Scaffolding
In the middle of the continuum, the child life specialist takes a more active role during the play itself while continuing to support the child’s initiative and interests. This includes asking questions, making comments, and extending the child’s play as suggested for facilitating guided play (Weisberg et al., 2016). Interactive scaffolding may also include child life specialists engaging in play alongside the child, previously described as the co-player role (Enz & Christie, 1997) or collaborative play (Pyle & Danniels, 2017). A range of play opportunities, from normative developmental play to therapeutic activities to exploratory medical play, may be facilitated at this level of adult involvement. The key feature is that the child life specialist carefully balances providing some guidance with supporting the child’s autonomy, remaining responsive to the child’s shifting interests and engagement. Thus, though child life specialists may have additional goals, such as socialization, emotional expression, or familiarization with medical equipment, the primary goal for activities within this guided play range is to support the child’s sense of mastery and control.
Case example. Twelve-year-old Mari has been hospitalized for several months in contact isolation. Mari expresses frustration with being stuck in her room and has begun to reject activities she previously enjoyed, most recently refusing to play her favorite board game because “we already played that a thousand times.” The child life specialist responds, “I get that. You’re practically a board game expert by now. I wonder if you could invent a new game?” Mari is excited about this possibility but unsure where to start, so the child life specialist asks open-ended questions to help her brainstorm. Over several days, Mari develops the game play cards with the child life specialist offering feedback to extend and clarify her ideas. Mari decides she will draw the new game board and delegates the task of making game pieces out of medical supplies to the child life specialist. When the game is ready, Mari is eager to invite her medical team to play.
Structured Play
As the continuum advances to structured play, the adult exerts a greater degree of control. Similar to playful learning and learning games (Pyle & Danniels, 2017; Zosh et al., 2018), structured play activities are designed by the child life specialist with specific goals in mind, goals which may take precedence over the child having a greater degree of choice in how to play. Adult behaviors in structured play are similar to what Bolig described as an environmental organizer (Bolig et al., 1986; Bolig & Gnezda, 1984) and include using suggestions, closed-ended questions, limited choices, and positive reinforcement to guide the child’s play. Child life specialists may engage at this higher level of direction when the child requires more support in the health care setting (e.g., patient is newly diagnosed) or when there is a need to guide the child toward a specific goal (e.g., expressing and labeling emotions). Therapeutic play and medical play may often fall within this category, though the defining feature is how closely the adult directs the situation to maintain the child’s focus on the activity.
Case example. The child life specialist receives a referral to meet Brooklyn, the 9-year-old sibling of a child receiving hospice services. Brooklyn’s parents have noticed she has been quieter than usual and are worried she may not be sharing her feelings about her brother’s worsening health. The child life specialist introduces an expressive art activity with colorful buttons and pom-pom balls and demonstrates how they will use these two materials to create a three-dimensional picture. The child life specialist explains the “hot buttons” are situations that make us feel angry, frustrated, scared or sad. The child life specialist offers examples and asks leading questions to help Brooklyn identity her “hot buttons” and decide where on the picture to glue them. Then the child life specialist explains “warm fuzzies” are what helps us feel happy or comforted and facilitates conversation about what might help Brooklyn with some of the challenges she identified. When the art project is complete, the child life specialist encourages Brooklyn to share it with her parents.
Directive Play
At the far end of the continuum, directive play encompasses situations where a child may be so emotionally overwhelmed or traumatized that they do not voluntarily engage in play. Again, drawing on the work of Bolig and colleagues (1984), the child life specialist seeks to establish a sense of trust and predictability for the child by providing structured materials, giving specific directions, and modeling expected behaviors. In contrast to structured activities that are intentionally designed and guided by the child life specialist with various goals, structured materials are pre-set activities, like puzzles or craft kits, which provide a sense of normalcy and an immediate experience of success. Directive play may commonly be used by child life specialists to establish quick rapport with children who are demonstrating high anxiety, distress, or withdrawal. This level of adult involvement may also be evident in play that occurs as part of distraction during procedures, as the child life specialist works to direct the child’s attention and engagement. A more extreme example of directive play would be “playing for” a child, a technique used to help children physically or emotionally unable to engage in play to vicariously experience play through the child life specialist (Gaynard et al., 1990).
Case example. Samuel is a five-year-old who has been in the intensive care unit for several weeks. Samuel’s health condition has stabilized, but he remains quiet and withdrawn, rarely verbalizing or showing interest in toys. After talking with Samuel’s family about his favorite activities, the child life specialist provides a superhero-themed sticker book. The child life specialist holds up the sticker sheet for Samuel to see and asks him to point to which sticker they should put on the page. At first, Samuel looks but does not respond. The child life specialist points to each sticker one by one, naming the characters, until Samuel nods. The child life specialist narrates, “Great choice! This picture needs Spiderman. Let’s put it right here.” The child life specialist points to the sticker sheet again and asks, “Which sticker do we need next?” The same routine of pointing to the stickers is repeated until Samuel nods. The child life specialist removes the sticker from the backing and asks, “Can you show me where it needs to go?” Samuel reaches for the sticker with a shaking hand, and the child life specialist helps him place it on the page.
Implications for Practice
It is important to recognize that the child life specialist’s level of involvement in play is fluid and frequently shifts between the levels described. For instance, a child admitted following an unexpected surgery may benefit initially from directive play with the child life specialist to build rapport and restore a sense of safety in this new environment. A structured play activity, like a sticker scavenger hunt on the way to the playroom, may support the medical goal of walking after surgery. In the playroom, the child life specialist may alternate between nondirective observation and environmental scaffolding as the child explores what to play and the child life specialist assesses that they would benefit from opportunities for choice and control. The child life specialist’s ongoing assessment of the child’s needs is paramount, as is their ability to sensitively adjust their behavior and level of involvement as the situation changes. Thus, it is essential to create tools like this expanded continuum of play that can support emerging professionals in understanding the wide range of strategies available for responding to children’s play and recognizing how child life play interventions are grounded in intentional decisions about how much direction would benefit the child.
The proposed continuum of adult involvement in play may also help address concerns about distinguishing play from child life interventions that are not play. The concern in using play to meet a specific, adult-driven outcome is that the child does not have freedom to choose their participation in or the ongoing direction of the activity, suggesting the activity is no longer play (Bolig et al., 1991; Brown, 2007). Theoretically, teaching, preparation, and procedural distraction that are initiated and fully directed by a child life specialist fall outside the continuum of play. In practice, however, child life interventions rarely, if ever, fit neatly into one category. Distraction often involves the child’s active participation in play, whether that is sensorimotor play with a light spinner or a game with rules on a tablet. A preparation session may shift between teaching and medical play as the child life specialist assesses the patient’s need for control as well as education. Rather than attempt to categorize activities across dichotomies – directive or nondirective, structured or unstructured, free play or therapeutic – the proposed continuum focuses on how adjustments in adult behavior shift control toward or away from the child and emphasizes the interaction between adult behavior and the goal of the activity. By referencing the continuum, child life specialists can ensure their actions are in line with their overall goals for the interaction as well as understand how to adjust their own involvement responsively to better meet the child’s needs.