Introduction
Certified Child Life Specialists (CCLSs) are essential in supporting children and families through challenging healthcare experiences (Romito et al., 2021). However, the demanding nature of their work often exposes them to trauma, grief, and bereavement, putting them at risk for workplace stress, compassion fatigue, and burnout (Ginter, Dumas, et al., 2024; Lagos et al., 2022). A growing body of literature has found that access to peer and direct supervisor support is one way to counteract emotionally straining work environments. Researchers found that CCLSs reporting a high-quality relationship with their direct supervisor had the strongest association with lower burnout and emotional exhaustion (Hoelscher & Ravert, 2021). Additionally, a study of community mental health nurses found that lower levels of burnout are reported when effective clinical supervision is implemented (Edwards et al., 2006).
The Association of Child Life Professionals (ACLP) recommends that CCLSs receive regular, ongoing clinical supervision to process clinical challenges, reduce compassion fatigue, promote professional growth, and ensure competent care for patients and families (ACLP, n.d.). Despite this recommendation, the lack of systematic organizational oversight of child life programs across the United States means there is no consistent record of which healthcare organizations provide access to clinical supervision and other employee supports. Furthermore, even in hospitals that offer clinical supervision, there is no available evidence measuring the efficacy of these programs for their intended purposes.
Literature Review
Child life specialists are vulnerable to the impacts of a highly emotionally demanding job, which can lead to burnout. Burnout has been identified among a variety of healthcare professionals, and CCLSs are no exception (Dyrbye et al., 2017). Holloway & Wallinga (1990) reported that child life professionals had lower burnout scores than Hoelscher & Ravert (2021) identified 30 years later. Hoelscher & Ravert (2021), found that the average burnout score in their sample was moderate. In a recent study of child life professionals who had been practicing for 5 years or less, 95% of participants reported experiencing burnout and did not expect to feel burnout at such an early point in their career (Ginter, Dumas, et al., 2024). The increase in experiences of burnout from 1990 to 2024 may indicate that burnout among CCLSs may be increasing over time. Of note, the Ginter et al. study (2024) was conducted during the Covid-19 pandemic, which could have affected burnout rates, however, when compared with a similar study conducted prior to the COVID-19 pandemic, the rate of CCLSs at risk of developing burnout or compassion fatigue was still high at 75% (Brinson, 2012).
Child life programs in hospital settings often cite a lack of resources and low pay for CCLSs as significant and persistent stressors, which can lead to burnout (Ehinger & Bales, 2023; Ginter, Dumas, et al., 2024). Burns-Nader et al. (2024) found that feelings of burnout among CCLSs were associated with low compensation, lack of professional respect, and ineffective leadership, while motivation to remain in the field was linked to supportive leadership that fostered recognition, provided resources, and encouraged the development of individual strengths. Given these findings, it is vital to identify potential solutions for CCLSs. A supportive and effective clinical supervision program may positively impact CCLS’s professional quality of life by offering consistent guidance, emotional support, and opportunities for reflective growth, key factors in reducing burnout and enhancing job satisfaction.
Clinical supervision programs are utilized in a variety of disciplines including nursing, social work, and clinical psychology. In nursing, there is mixed evidence for the effectiveness of clinical supervision, with some studies observing no differences, while others report higher levels of perceived support and lower levels of burnout (Hyrkäs, 2005; Koivula et al., 2000; Teasdale et al., 2001). However, a systematic review by Rothwell et al. (2021) identified several studies demonstrating connections between effective clinical supervision and positive outcomes in workplace settings. For example, several studies provided evidence for an increase in job satisfaction and well-being, in addition to clinical supervision decreasing stress and anxiety (Rothwell et al., 2021). In a qualitative study of 38 allied health professionals, the organization’s focus on prioritizing supervision was highlighted as one of three major themes related to the overall success and effectiveness of the program (Snowdon et al., 2020). Additionally, in a study conducted with community mental health nurses, those who participated in effective clinical supervision reported lower levels of burnout (Edwards et al., 2006). It is vital to continue to explore the potential efficacy that supervision can have on the professional quality of life of healthcare workers.
Clinical Supervision and the Child Life Profession
Clinical supervision in the child life profession is “a formal process based on a clinically focused professional relationship between the practitioner and supervisor/facilitator to support and enhance the quality of care for patients and families” (ACLP, n.d.). Effective supervision occurs when, according to the ACLP, there is a formal, supportive relationship that fosters reflective practice, critical thinking, and therapeutic competence among practitioners (ACLP, n.d.). In the context of child life, clinical supervision is a reflective process focused on supporting emotional well-being, ethical decision-making, and professional growth through guided, collaborative dialogue. This is different from administrative supervision, which centers on job performance and task management. Rather than reporting to a manager, clinical supervision offers a structured space for CCLSs to explore their clinical experiences, process challenges, and strengthen therapeutic competence in a supportive, non-evaluative setting.
To date, very few studies have explored the implementation and efficacy of clinical supervision related to professional quality of life for pediatric healthcare workers, and none have looked at outcomes for CCLSs specifically. In a study of 196 CCLSs, 51.3% of participants reported that they had never received clinical supervision from another child life specialist, suggesting disparities in access to what may be a useful employee wellbeing resource (Lagos et al., 2022). Traditional in-person clinical supervision in the field of child life is often implemented at the discretion of program leadership. Therefore, research on clinical supervision within the child life profession is limited.
The ACLP Position Statement on Clinical Supervision (2018) includes several older foundational works, many of which are not specific to child life or focus primarily on student and early career development rather than post-certification professionals. While texts such as Supervision in Child Life (Rode, 2005) provide helpful insights, they focus on intern development rather than long-term professional support. Other cited works (e.g., Campbell, 2000; Hawkins & Shohet, 2007; Malchiodi & Riley, 1998) come from counseling or medical contexts, underscoring the lack of recent, child life-specific research on clinical supervision. This gap highlights the need to explore formal clinical supervision experiences among CCLSs post-certification.
Barriers to Clinical Supervision
While the potential benefits of clinical supervision have been cited in a variety of professions, there are barriers to its implementation. Notably, in-person clinical supervision facilitated by the employer for mental health professionals has revealed several challenges, including unclear definitions of clinical supervision, the potential for informal peer support to be as effective as formal supervision, perceptions of supervision as punitive, and issues with time, cost, and a lack of standardized training for facilitators (Spence et al., 2001). Similarly, in social work, supervision has been critiqued for lacking clear structure and consistent outcomes, especially when not grounded in reflective practice (Beddoe, 2010). In clinical psychology, studies have emphasized the importance of supervisory alliance and structured reflection but also note inconsistencies in training and evaluation standards across programs (Watkins, 2011).
A scoping review of clinical supervision within the nursing profession further supports these findings, reporting no universally accepted definition of clinical supervision and lack of consensus on an appropriate model for providing clinical supervision (Masamha et al., 2022). These challenges mirror concerns in the child life profession (Ginter, Cahlander, et al., 2024) where supervision practices vary significantly across institutions and research has not been conducted to define best practices.
Edwards et al. (2006) highlighted an additional challenge of clinical supervision, which is the ability to set aside time for supervision amid clinical responsibilities. Despite the growing body of research that shows the potential benefits of clinical supervision, it can be challenging to find the time, resources, and appropriate support to implement a high quality, positive clinical supervision experience in a healthcare setting (Masamha et al., 2022).
Additionally, CCLSs work in a growing number of non-hospital environments such as schools, private practice, non-profit organizations, disaster relief, rehabilitation, and other areas where children may be experiencing challenges. Little is known about what options CCLSs in community settings have to access clinical supervision support. The ACLP statement on child life in community settings highlights the ethical importance of access to supervision for those practicing outside of the hospital, yet no such formal program has been offered (ACLP, 2018).
Virtual Clinical Supervision
The use of technology to facilitate virtual clinical supervision has expanded significantly in recent years, offering numerous benefits across various health professions. While earlier work by Rousmaniere (2014) noted benefits such as increased availability, reduced cost, and greater flexibility, more recent studies have highlighted the crucial role virtual supervision has continued to play in maintaining professional support. In the health profession fields (e.g., counseling and nursing), virtual supervision has been recognized for increasing accessibility, improving communication between supervisors and supervisees, and providing timely support (Geller et al., 2023; Harada et al., 2025).
For child life programs that struggle to provide consistent, high-quality clinical supervision amidst a wealth of other clinical and administrative responsibilities, this type of programming in a virtual environment could circumvent the challenges with in-person supervision and potentially decrease the workload of supervisors currently providing this service. Also, child life programs without the resources to offer adequate clinical supervision could potentially have a new opportunity to provide much-needed support to professionals.
Recognizing these problems, the present study aimed to explore the impact of a group virtual clinical supervision program on the professional quality of life (ProQOL) for CCLSs working in healthcare and community settings. This study sought to provide valuable insights into the potential benefits of group virtual clinical supervision and its impact on professional quality of life indicators, such as burnout, secondary trauma, and compassion fatigue, while also providing a foundation for continued exploration.
This study was guided by two primary research questions:
-
What effect does participation in a virtual group clinical supervision program have on the professional quality of life of CCLSs?
-
Do certain factors (i.e. work status, length of time in the field, workplace setting, etc.) influence the efficacy of clinical supervision programs for CCLSs.
The second research question was not addressed in this analysis due to the statistical limitations of a small sample size. Only the first research question will be addressed in this exploratory study.
Method
Participants and Procedures
Prior to implementation of the study, Institutional Review Board approval was sought and obtained at a large public university. This study used a convenience sample of CCLSs who were already enrolled in a virtual clinical supervision program. The program was provided via Zoom and offered as part of a paid membership to an online community of CCLSs. The cost to be a part of the community is $19.99/month and includes access to professional development and networking opportunities. Members of the paid community are offered the opportunity to participate in the clinical supervision program at no added cost.
A total of six cohorts completed the virtual clinical supervision program in this study, with cohort sizes of four to five specialists and one supervision leader. The first two cohorts of the virtual supervision program were 12 weeks in length and participants met every other week for 60 minutes (e.g., 6 total sessions). The last four cohorts of the virtual supervision program were 16 weeks in length and met every other week for 60-75 minutes (e.g., 8 total sessions). Participants were assigned to supervision groups based on scheduling availability, length of time in the paid community, and whether they had completed supervision with this community in the past so that those who had not yet received supervision were given priority.
The virtual clinical supervision program was led by two CCLSs with extensive experience providing clinical supervision. The first child life specialist has been certified for 31 years and has been providing one-on-one clinical supervision support for 15 years. The second child life specialist has been certified for 19 years and has been providing clinical supervision for seven years. While each supervisor structured sessions differently, all sessions were in alignment the ACLP’s guidelines of ensuring it was a reflective process focused on supporting emotional well-being, ethical decision-making, and professional growth through guided, collaborative dialogue. CCLSs in this study might have interacted with their clinical supervisor outside of designated supervision sessions through the online community, such as by attending the same live webinars or engaging in discussion threads and post comments.
Once enrolled in the supervision program, participants were informed of the study and invited to participate via an email distributed by the research team. The email contained a link to study materials. Those interested visited the link and provided electronic consent. Once electronic consent was obtained, participants completed a survey that gathered information about the background of participants and their professional quality of life. The survey was completed again following the completion of the virtual clinical supervision program. Twenty-four CCLSs were invited to participate in the study. All participants initially consented to participate but two participants did not complete both pre- and post-surveys and thus were removed from the study. It is important to note that five CCLSs participated in two supervision cohorts during the data collection period and could therefore have submitted responses to the surveys at two different time points. This is further addressed in the limitations section.
Measures
Demographic and Workplace Factors
The participants provided demographic and workplace information, including age, gender, ethnicity, length of time as a child life specialist, length of time in their current role, position status (i.e., part-time, full-time, or PRN), work setting (i.e., healthcare or non-healthcare), US region, and whether they have pursued professional development opportunities focused on clinical supervision in the past.
Professional Quality of Life Scale for Health Workers
To measure professional quality of life, participants completed the Professional Quality of Life for Health Workers measure (ProQOL Health; Stamm, n.d.), which measures compassion satisfaction, perceived support, burnout, secondary traumatic stress, and moral distress. The ProQOL Health includes 30 items that assess how frequently a healthcare worker has experienced a positive or negative situation or feeling in the last 30 days (e.g., “Because of my work, I have unwanted, distressing thoughts” and “I am happy that I chose to work in healthcare”). Participants provided responses on a Likert scale from 1 = “Never” to 5 “Very often.”
Subscale scores were created by totaling subscale items. For all subscales, a score of 6-12.4 is considered “low”, a score of 12.5-23.4 is considered “moderate”, and a score at or above 23.5 is considered “high”. The subscales were compassion satisfaction (CS; α = 0.788), perceived support (PS; α = 0.734), burnout (BO; α = 0.751), secondary traumatic stress (ST; α = 0.802), and moral distress (MD; α = 0.633). Cronbach alpha values were calculated from the participants’ pre-program survey responses.
Data Analysis
Analyses were conducted in R (version 4.3.2). Descriptive statistics were conducted to describe the demographic characteristics of participants and ProQOL Health scales. To examine the research question, paired t-tests were conducted to evaluate the difference between pre-and post-program scores for each of the five ProQOL Health subscales. All five t-tests were run with an alpha level of .05 to determine significant differences. To avoid risk of Type 1 errors, any significant differences between pre-and post-program scores were corrected for multiple comparisons by adjusting this alpha value (Chen et al., 2017).
With a complete sample size of 22 participants and six work factors to explore, a multiple regression analysis could not be conducted to determine how work factors influenced program effects on professional quality of life, as the sample size was insufficiently powered to accurately explain this influence (Maxwell, 2000). Additionally, no ANOVA tests were conducted for the categorical demographic or work factors on changes in subscale scores following the program. With a smaller sample size distributed across several levels, most demographic or work variables did not have enough participants per category level required to run a one-way ANOVA, much less a multivariate ANOVA to account for multiple dependent variables simultaneously. Further consideration of analysis limitations and future directions are addressed in the discussion.
Results
A total of 24 CCLSs participated in the clinical supervision program in 2023, and 22 had a complete data set; thus this analysis included 22 responses (Table 1). All participants identified as female (n = 22, 100%) with 86% of participants identifying as White. Forty percent (n=9) of participants were between the ages of 20 to 30 years, 36% (n=8) of participants were between the ages of 31 to 40 years, and 23% (n=5) were 41 years of age or older. Several participant workplace factors were also recorded (Table 2). Fifty-nine percent (n=13) of participants had been certified for less than 10 years, while the other 41% percent (n=9) had been certified for 10 years or more. Of the participants, 32% percent (n=7) had previously pursued clinical supervision, and 18% (n=4) had completed clinical supervision rounds.
Impact of Virtual Clinical Supervision on the Professional Quality of Life of CCLSs
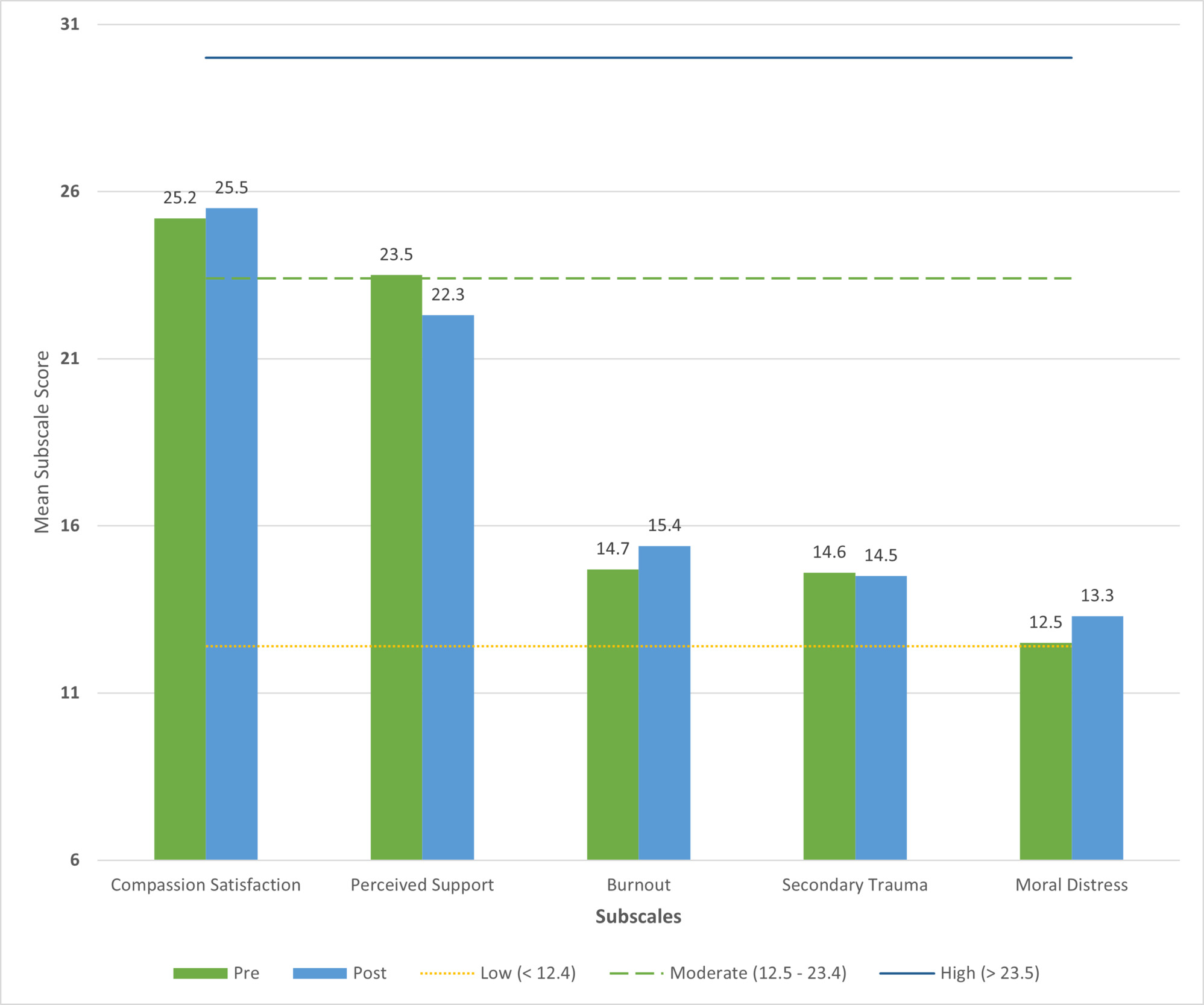
Prior to completing the virtual clinical supervision program, mean participant scores on the compassion satisfaction (M= 25.2) and perceived support (M= 23.5) subscales of the ProQoL Health fell within the “high” category. Additionally, burnout (M= 14.7), secondary trauma (M=14.6), and moral distress (M=12.5) scores fell within the “moderate” category prior to the program. After completing the program, mean participant scores remained in the same high and moderate categories except for perceived support (M = 22.3) which was within the moderate category following the program.

A paired samples t-test was conducted for each of the five ProQOL Health subscales to compare the scores before and after the virtual clinical supervision program participation (Table 3). The pre-program and post-program scores were not significantly different for compassion satisfaction (p = .683), perceived support (p = .131), burnout (p = .511), secondary trauma (p = .801), or moral distress (p = .125). As these scores were not significantly different at an alpha of .05, multiple comparison correction was not conducted.
Discussion
This is the first study to explore virtual clinical supervision for CCLSs, with a particular focus on the role of a virtual group clinical supervision program for CCLSs professional quality of life. The findings revealed that overall ProQOL Health scores did not significantly change following the 12 and 16-week programs, suggesting that short-term engagement in virtual supervision may not produce measurable improvements in general professional quality of life. However, there were several ProQOL Health subscales in which the participants on average demonstrated high compassion satisfaction and perceived support prior to participating in the clinical supervision program. Therefore, the average child life specialist that participated in this study may have less of a need to improve their professional quality of life; this highlights a need to explore other factors that may influence their need and ability to improve during a supervision program.
Overall, the findings underscore several important insights related to professional quality of life, and the need to continue exploring the potential for virtual programs to address some of the challenges identified by both the child life profession and related fields. Burnout is a significant issue in the child life profession (Burns-Nader et al., 2024; Ginter, Dumas, et al., 2024). This aligns with the current study’s findings that burnout remains a concern, as CCLSs, on average, demonstrated moderate levels of burnout both prior to and after participating in the program. These findings point to the need for mitigating burnout in the child life field and therefore highlight that further exploration of effective interventions for burnout should be considered in future program design.
Limitations
This study has limitations that should be noted. The sample size in this study is small, resulting in analysis that is sufficiently powered to explore differences between pre- and post-program scores, but not sufficient to analyze the influence of workplace factors on program effectiveness. Because data were collected anonymously, it is not possible to confirm whether a small number of participants may have completed the survey in more than one cohort. Based on the available identifiers, we estimate that up to five individuals could have participated more than once; additionally, two responses in our sample did not submit complete data and were excluded from analysis, further challenging the opportunity to identify repeats. Given the small number and the exploratory nature of the study, any potential overlap is unlikely to have significantly impacted the findings; however, this should be considered when interpreting results. The sample also includes only females who were predominantly white, which limits the generalizability of the results. To make the results more generalizable, it would be beneficial to include participants who identify as other genders as well as participants of a variety of ethnicities. Another limitation is the length of the supervision program. There is a possibility that six or eight sessions of supervision may not be sufficient to see the impact of the program. Because every participant received supervision as part of the program, the study did not include a comparison group of CCLSs without supervision. Participants in this study paid to be a part of a community that also offers supervision, which can impact their overall engagement in the program. This supervision was also done virtually, whereas many group clinical supervision programs are in-person formats.
Further research is needed to determine whether there are variations in effectiveness of an in-person format versus a virtual format for clinical supervision programs. Additionally, this virtual format increases the likelihood that participants were not peers from the same organization, which is a deviation from the typical method of receiving group clinical supervision and could impact its overall effectiveness. Since there were two supervision leaders, it is possible that there are differences in effectiveness based on the supervision leader.
Implications
Broader trends in healthcare and education include providing virtual programming, and this has become more prevalent since the COVID-19 pandemic (Anthony Jnr & Noel, 2021; Makda, 2025; Olson et al., 2002). Offering a virtual clinical supervision program could have positive impacts on child life professionals. Barriers to clinical supervision, such as time constraints, cost, and a lack of standardized training, are well-documented across professions (Spence et al., 2001). Virtual supervision offers a potential solution to these challenges, as it provides greater accessibility and flexibility, particularly for CCLSs working in non-hospital settings. Virtual supervision programs could also reduce the burden on professionals currently responsible for providing in-person supervision, thereby enhancing the consistency and quality of support available to CCLSs.
Future clinical supervision programs should focus on measuring the efficacy of their program and identifying the specific needs of their participants to tailor the program to meet those needs. Healthcare systems and other organizations providing supervision should continue to address the role of their program on professional quality of life and continue to measure the impact that supervision programs have on their staff while adjusting the structure to meet the needs of CCLSs.
Future Research
Future research should strongly consider the addition of a control group to identify potential differences between those receiving supervision versus those who are not. The addition of a control group would help to explore the potential benefits of participating in a supervision program and the possible challenges CCLSs may experience in reference to their professional quality of life if they are not participating in any supervision. In the future, a larger sample size would provide the ability to run regression analyses and ANOVAs to explore the associations between workplace factors and ProQOL Health, control for confounding variables, and compare change in scores over time. Additionally, more longitudinal research on the impacts of clinical supervision should be considered to examine direct impacts on retention and ProQOL Health, comparing the effects of spending time in clinical supervision programs to the general effect of working in the field across time without direct program participation. It is important to note that participants were assigned to one of two supervisors. Exploring variations in scores as it relates to the supervisor relationship would also add beneficial information on this relevant topic. Lastly, future research should consider the benefits and challenges of a virtual implementation of supervision versus in-person supervision programs.
Conclusion
CCLSs are vulnerable to the impacts of a highly, emotionally demanding job. This study examined the relationship between a virtual clinical supervision program and professional quality of life. The participating CCLSs demonstrated high compassion satisfaction and perceived support before starting clinical supervision. While this exploratory study did not find clinical supervision to have a significant impact on pre and post ProQOL Health scores, the CCLSs in the study demonstrated moderate levels of burnout both before and after the clinical supervision program, highlighting an important focus in the field where burnout rates are high, and turnover is frequent (Hoelscher & Ravert, 2021). It is unclear if specific work factors present unique needs for improving professional quality of life, and the identification of potential unique needs and the efficacy of clinical supervision programs in addressing these needs should be further explored. Given the persistent presence of burnout in the field, further examination of how supervision programs can be structured to meet the evolving needs of CCLSs remains a critical area of inquiry.
Disclosure Statement
Two authors were involved in the logistical execution of the virtual clinical supervision program, but did not lead or participate in any of the supervision programming. Additionally, neither author was involved in the data analysis process.
Funding Statement
This supervision program was created and implemented by Child Life On Call, LLC. While author one and author three were employed by the company at the time of this study, the participants in this study did not directly pay the authors for this program nor did the company provide financial support for the analyses or manuscript.